

Intravascular extension of Wilms tumor
- PMID: 11420491
- PMCID: PMC1421956
- DOI: 10.1097/00000658-200107000-00017
Intravascular extension of Wilms tumor
Abstract
Objective: To define the incidence and manifestations of and optimal therapy for children with intravascular extension of Wilms tumor.
Methods: Children on a collaborative study of Wilms tumor who had intravascular extension into the inferior vena cava (IVC) or atrium were identified. Surgical checklists and surgical and pathology reports were reviewed.
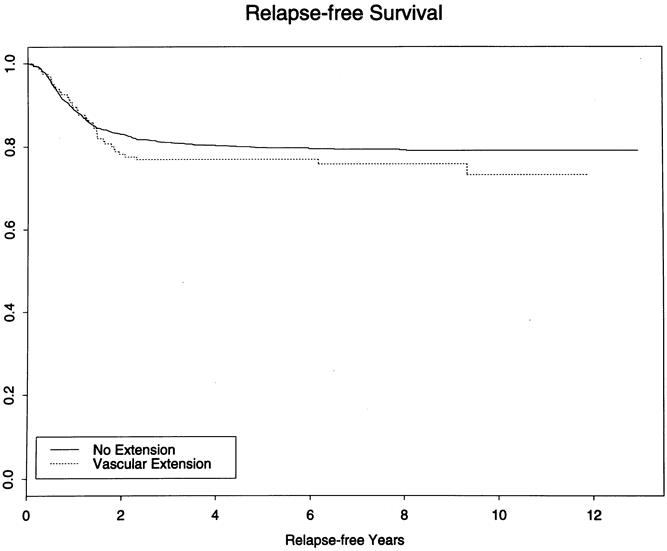
Results: One hundred sixty-five of 2,731 patients had intravascular extension of Wilms tumor. The level of extension was IVC in 134 and atrium in 31. Sixty-nine had received preoperative therapy (55 with IVC extension and 14 with atrial extension) for a median of 8 weeks. Complications during preoperative chemotherapy were seen in five patients (tumor embolism and tumor progression in one each, and three with adult respiratory distress syndrome, one of which was fatal). The intravascular extension of the tumor regressed in 39 of 49 children with comparable pre- and posttherapy radiographic studies, including 7 of 12 in whom the tumor regressed from an atrial location, thus obviating the need for cardiopulmonary bypass. Surgical complications occurred in 36.7% of the children in the atrial group and 17.2% in the IVC group. The frequency of surgical complications was 26% in the primary resection group versus 13.2% in children with preoperative therapy. When all the complications of therapy were considered, including those that occurred during the interval of preoperative chemotherapy (one of the five also had a surgical complication), the incidence of complications among those receiving preoperative therapy was not statistically different from the incidence among those who underwent primary resection. The difference in 3-year relapse-free survival (76.9% for 165 patients with intravascular extension, 80.3% for 1,622 patients with no extension) was not statistically significant whether or not it was adjusted for stage and histology.
Conclusions: Preoperative treatment of these children may facilitate resection by decreasing the extent of the tumor thrombus, but the overall frequency of complications is similar in both groups.
Figures
References
-
- Green DM, Breslow NE, Beckwith JB, et al. Comparison between single-dose and divided-dose administration of dactinomycin and doxorubicin for patients with Wilms tumor: a report from the National Wilms Tumor Study Group. J Clin Oncol 1998; 16: 237–245. - PubMed
-
- Ritchey ML, Kelalis PP, Breslow N, et al. Intracaval and atrial involvement with nephroblastoma: review of National Wilms’ Tumor Study 3. J Urol 1988; 140: 1113–1118. - PubMed
-
- Ritchey ML, Kelalis PP, Breslow N, et al. Surgical complications after nephrectomy for Wilms’ tumor. Surg Gynecol Obstet 1992; 175: 507–514. - PubMed
-
- Wagget J, Koop CE. Wilms’ tumor: preoperative radiotherapy and chemotherapy in the management of massive tumors. Cancer 1970; 26: 338–340. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
