

Public health impact of adverse bone effects of oral corticosteroids
- PMID: 11422020
- PMCID: PMC2014495
- DOI: 10.1046/j.0306-5251.2001.1385.x
Public health impact of adverse bone effects of oral corticosteroids
Abstract
Aims: The objective of this study was to estimate the number of fractures attributed to oral corticosteroid use.
Methods: Information was obtained from the General Practice Research Database which contains medical records of general practitioners in the UK. The total number of corticosteroid-related fractures during a course of treatment was estimated using the formula for attributable risk among the exposed.
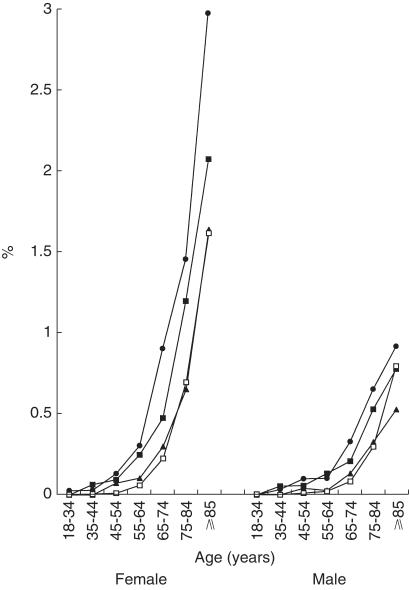
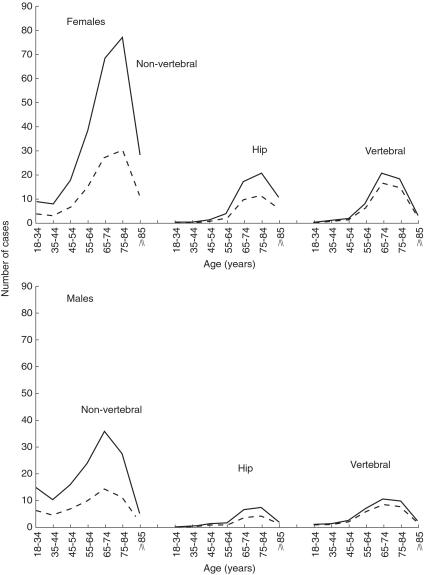
Results: A total of 244 235 patients was prescribed an oral corticosteroid. The rate of hip fractures increased exponentially with age in both males and females. The excess number of hip fracture cases among females aged 85 years or older using 7.5 mg prednisolone per day or more was 1.4 cases per 100 patients per year. About 47% of all hip and 72% of all vertebral fractures that occurred can be attributed to oral corticosteroid use. Among 10 000 female users of higher doses, 99.7 nonvertebral, 31.6 hip and 45.8 vertebral fractures can be attributed to use of oral corticosteroids.
Conclusions: The targeting of high-risk patients will be important for implementing preventative strategies in a cost-effective manner.
Figures
Similar articles
-
Use of oral corticosteroids and risk of fractures.J Bone Miner Res. 2000 Jun;15(6):993-1000. doi: 10.1359/jbmr.2000.15.6.993. J Bone Miner Res. 2000. PMID: 10841167 Review.
-
Oral corticosteroids and fracture risk: relationship to daily and cumulative doses.Rheumatology (Oxford). 2000 Dec;39(12):1383-9. doi: 10.1093/rheumatology/39.12.1383. Rheumatology (Oxford). 2000. PMID: 11136882
-
The population risk of fractures attributable to oral corticosteroids.Pharmacoepidemiol Drug Saf. 2005 Mar;14(3):177-86. doi: 10.1002/pds.1075. Pharmacoepidemiol Drug Saf. 2005. PMID: 15672413
-
Oral glucocorticoid use is associated with an increased risk of fracture.Osteoporos Int. 2004 Apr;15(4):323-8. doi: 10.1007/s00198-003-1548-3. Epub 2004 Feb 5. Osteoporos Int. 2004. PMID: 14762652
-
Corticosteroid-induced osteoporosis.Nurs Clin North Am. 2001 Sep;36(3):455-66, ix. Nurs Clin North Am. 2001. PMID: 11532660 Review.
Cited by
-
Schistosoma mansoni Tegument (Smteg) Induces IL-10 and Modulates Experimental Airway Inflammation.PLoS One. 2016 Jul 25;11(7):e0160118. doi: 10.1371/journal.pone.0160118. eCollection 2016. PLoS One. 2016. PMID: 27454771 Free PMC article.
-
Prevention and treatment strategies for glucocorticoid-induced osteoporotic fractures.Clin Rheumatol. 2007 Feb;26(2):144-53. doi: 10.1007/s10067-006-0315-1. Epub 2006 May 3. Clin Rheumatol. 2007. PMID: 16670825 Review.
-
Guidance for the adjustment of FRAX according to the dose of glucocorticoids.Osteoporos Int. 2011 Mar;22(3):809-16. doi: 10.1007/s00198-010-1524-7. Epub 2011 Jan 13. Osteoporos Int. 2011. PMID: 21229233
-
Bone turnover decreases and bone structure improves during treatment with weekly high-dose methylprednisolone for 12 weeks in Graves' orbitopathy.Endocrine. 2023 Dec;82(3):664-672. doi: 10.1007/s12020-023-03494-5. Epub 2023 Sep 7. Endocrine. 2023. PMID: 37676399 Free PMC article.
-
Adverse Outcomes, Healthcare Resource Utilization, and Costs Associated with Systemic Corticosteroid use Among Adults with Systemic Lupus Erythematosus in the UK.Rheumatol Ther. 2023 Oct;10(5):1167-1182. doi: 10.1007/s40744-023-00566-w. Epub 2023 Jul 3. Rheumatol Ther. 2023. PMID: 37400682 Free PMC article.
References
-
- Adinoff AD, Hollister MD, Roger J. Steroid-induced fractures and bone loss In patients with asthma. N Engl J Med. 1983;309:601–607. - PubMed
-
- Dykman TR, Gluck OS, Murphy WA, Hahn TJ, Hahn BH. Evaluation of factors associated with glucocorticoid-induced osteopenia in patients with rheumatic diseases. Arthritis Rheum. 1985;28:361–368. - PubMed
-
- Hooyman JR, Melton Jl, IIII, Nelson AM, O'Fallon MW, Lawrence Riggs B. Fractures after rheumatoid arthritis. Arthritis Rheum. 1984;27:1353–1361. - PubMed
-
- McDougall R, Sibley J, Haga M, Russell A. Outcome in patients with rheumatoid arthritis receiving prednisone compared to matched controls. J Rheumatol. 1994;21:1207–1213. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
