

Drug therapy in the elderly: what doctors believe and patients actually do
- PMID: 11422022
- PMCID: PMC2014493
- DOI: 10.1046/j.0306-5251.2001.01401.x
Drug therapy in the elderly: what doctors believe and patients actually do
Abstract
Aims: To examine the medication adherence among old persons living in their own homes, to assess their knowledge of their medication, and to indicate target areas for intervention.
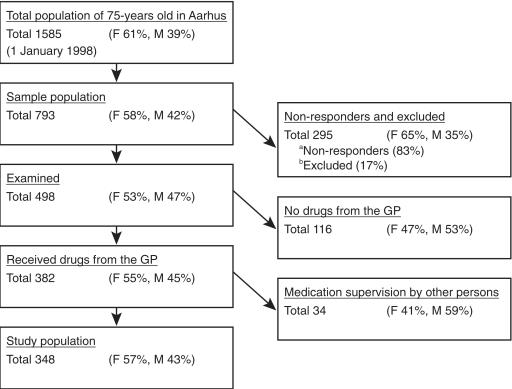
Methods: A cross-sectional study of data collected from randomly selected samples of 348 persons, aged 75 years recruited from a population-based register in the municipality of Aarhus, Denmark. Information on all drugs was collected from the subjects during a home visit, and their drug storage was examined. Information was collected from the general practitioners (GP). The measures of adherence were scores of agreements between the GPs' lists and the subjects' actual drug consumption.
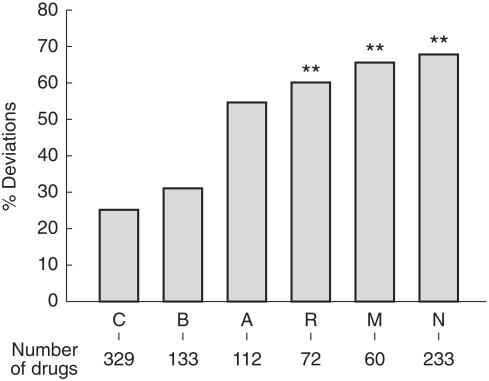
Results: We found disagreement between the drug information collected from the study population and from the GPs: concerning drugs in 22% of the study-population, concerning doses in 71%, and concerning regimens prescribed by the GP in 66%. Twenty-four percent stated that they did not always follow prescriptions. Most of the deviations from prescriptions were toward lower doses and less frequent drug intake. The drugs most often involved in deviations were hypnotics, analgesics, bronchodilators and diuretics. Sixty percent of the participants knew the purpose of medication, and 21% knew the consequences of omission of the drugs. Less than 6% of the subjects knew about the toxic risks, side-effects, or potential drug interactions. The participants' knowledge of the drugs was positively associated with their adherence. We found a correlation between an increased number of prescribed frequency of drug intake per day and deviation from the regimen (r = 0.25, P = 0.01). There was a positive association between nonadherence and the use of three or more drugs (odds ratio (OR) 2.5; 95% confidence interval (CI) 1.5,4.1), prescriptions from more than one doctor (OR 2.5; 95% CI 1.3,4.8), and probability of dementia (OR 9.0; 95% CI 1.1,72.5). Moreover compliance aids facilitated adherence (OR 4.4; 95% CI 1.6,12.3). Persons living alone were more prone to medication errors (OR 2.0; 95% CI 1.1,3.5).
Conclusions: A differentiated evaluation of adherence by considering the drug, the dose, and the regimen separately produced quantifiable data concerning the subjects' medication habits. Non-adherence ranged from 20 to 70% depending on the measuring method. The participants' knowledge of the treatment was poor. Our results suggest that better information on medication and the use of compliance aids may prevent nonadherence. Special attention should be paid to persons receiving three or more drugs, living alone, receiving drugs from other doctors, and to persons with predementia symptoms, as they are at higher risk of nonadherence.
Figures
References
-
- Col N, Fanale JE, Kronholm P. The role of medication noncompliance and adverse drug reactions in hospitalizations of the elderly. Arch Intern Med. 1990;150:841–845. - PubMed
-
- Bergman U, Wiholm BE. Drug-related problems causing admission to a medical clinic. Eur J Clin Pharmacol. 1981;20:193–200. - PubMed
-
- Sullivan SD, Kreling DH, Hazlet TK. Noncompliance with medications and subsequent hospitalization: a literature analysis and cost of hospitalization estimate. J Res Pharm Econ. 1990;2:19–33.
-
- Coons SJ, Sheahan SL, Martin SS, et al. Predictors of medication noncompliance in a sample of older adults. Clin Ther. 1994;16:110–117. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
