

The evaluation of two methods to facilitate shared decision making for men considering the prostate-specific antigen test
- PMID: 11422636
- PMCID: PMC1495230
- DOI: 10.1046/j.1525-1497.2001.016006391.x
The evaluation of two methods to facilitate shared decision making for men considering the prostate-specific antigen test
Abstract
Objective: California law (Grant H. Kenyon Prostate Cancer Detection Act) requires physicians to inform all patients older than aged 50 years who receive a prostate examination about the availability of the prostate-specific antigen (PSA) test. Physicians are not given guidance on how this information should be presented. We sought to evaluate the effects upon PSA screening rates of informing patients about PSA testing by 2 different techniques.
Design: Factorial comparison of discussion versus video formats for presenting information about the PSA test.
Setting: Patients were recruited through the Health Appraisal screening program in the Department for Preventive Medicine, Kaiser Permanente, San Diego, Calif.
Participants: Male patients undergoing health appraisal screening participated in 1 of 4 groups providing information about PSA screening: usual care ( n=43), discussion about risks and benefits of PSA ( n=45), shared decision-making video ( n=46), or video plus discussion ( n=42). Participants were sequentially assigned to 1 of the 4 groups.
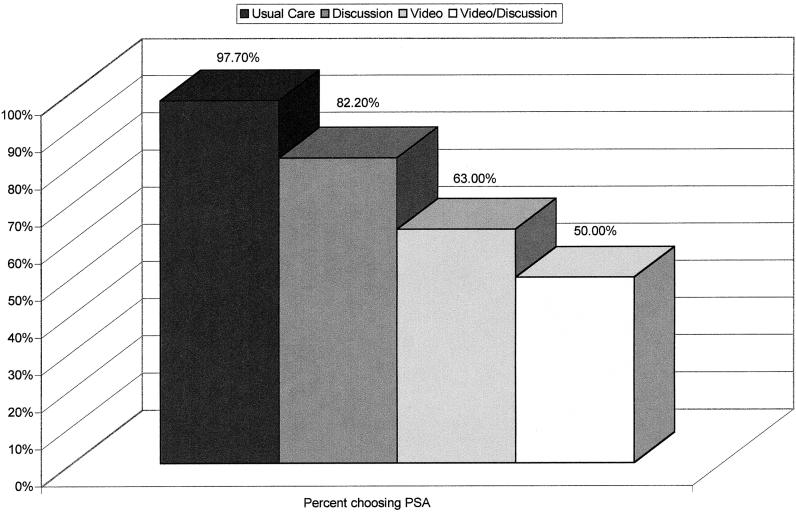
Results: No significant differences in demographics or family history was demonstrated between the groups at the time of group assignment. Participants in the intervention groups rated the information as clear, balanced, and fair. There were significant differences in the number of men requesting a PSA test, with the highest rate in the usual care group (97.7%), followed by discussion (82.2%), video (60.0%), and video plus discussion (50.0%).
Conclusion: Providing information about PSA screening in the form of video or discussion is feasible and significantly alters PSA screening rates.
Figures
References
-
- Boyle P. Prostate-specific antigen (PSA) testing as screening for prostate cancer: the current controversy. Ann Oncol. 1998;9:1263–4. - PubMed
-
- Barry MJ. PSA screening for prostate cancer: the current controversy — a viewpoint. Ann Oncol. 1998;9:1279–82. - PubMed
-
- Johansson JE, Holmberg L, Johansson S, Bergström R, Adami HO. Fifteen-year survival in prostate cancer. A prospective, population-based study in Sweden. JAMA. 1997;277:467–71. - PubMed
-
- The American Urological Association Prostate Cancer Clinical Guidelines Panel. Report on the Management of Clinically Localized Prostate Cancer. Baltimore, Md: American Urological Association Inc; 1995. - PubMed
-
- American Cancer Society Prostate Cancer Screening Guidelines. Cancer Facts and Figures 1997. Atlanta, Ga: American Cancer Society; 1997.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous