

Whipple's disease and "Tropheryma whippelii"
- PMID: 11432814
- PMCID: PMC88990
- DOI: 10.1128/CMR.14.3.561-583.2001
Whipple's disease and "Tropheryma whippelii"
Abstract
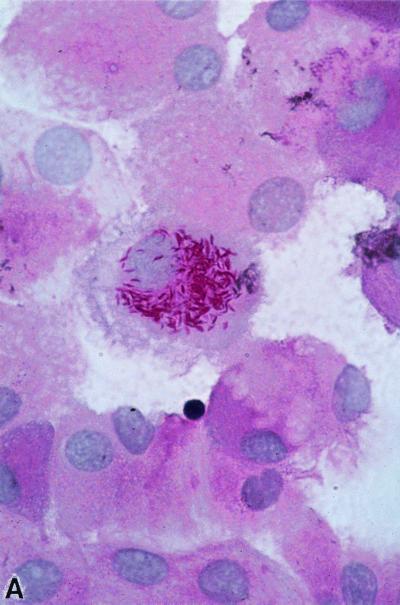
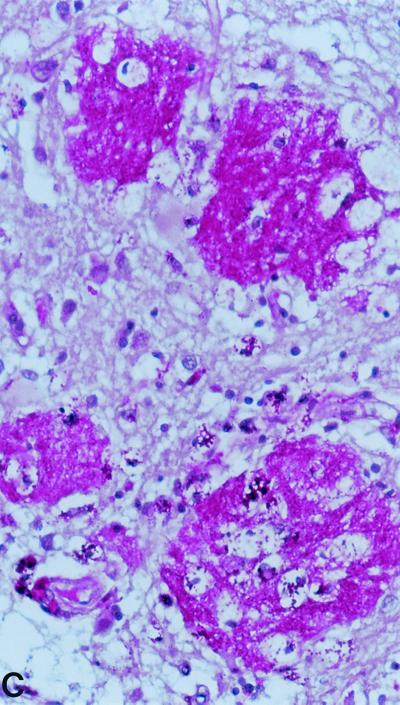
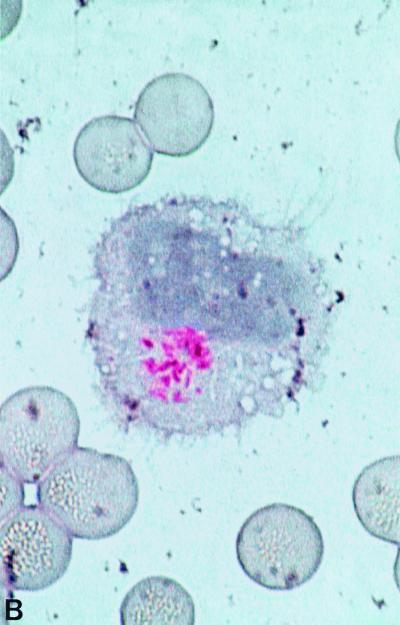
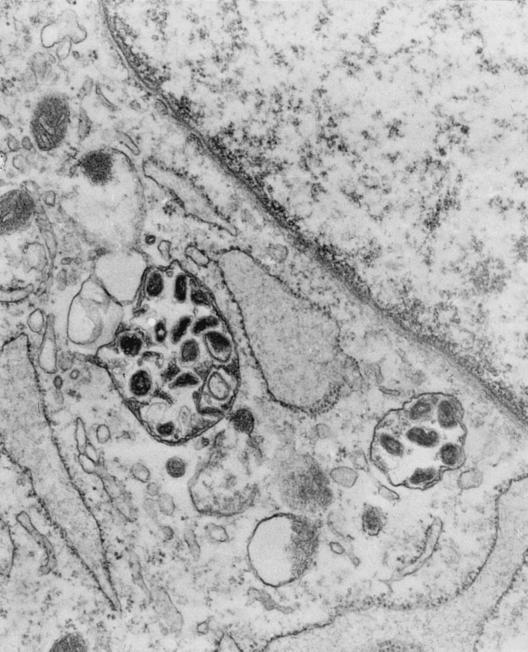
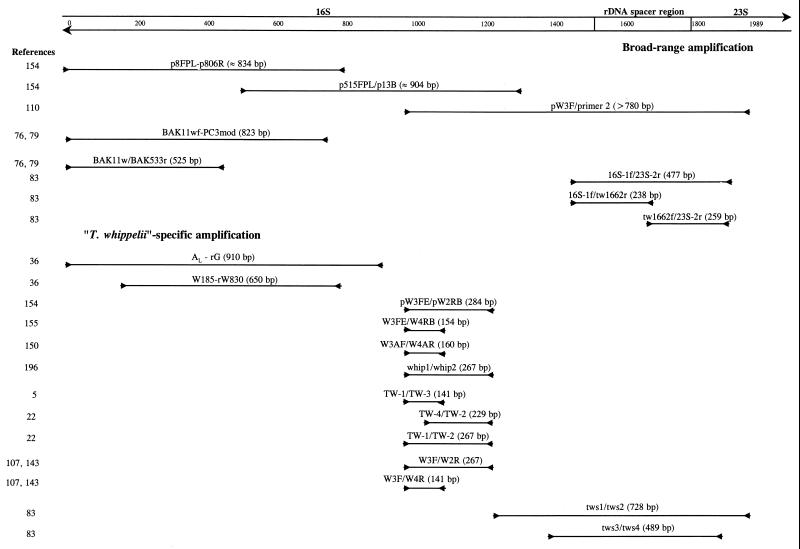
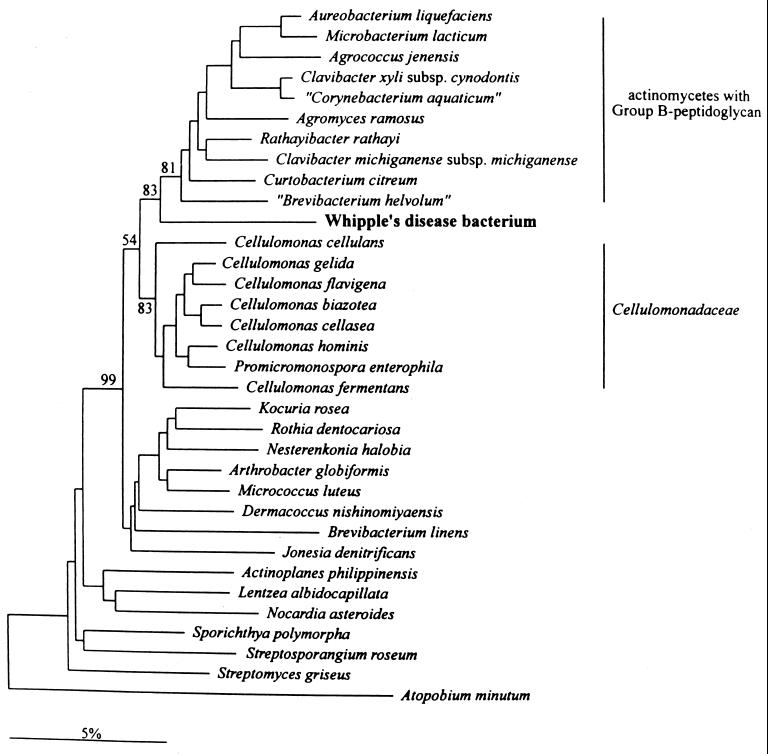
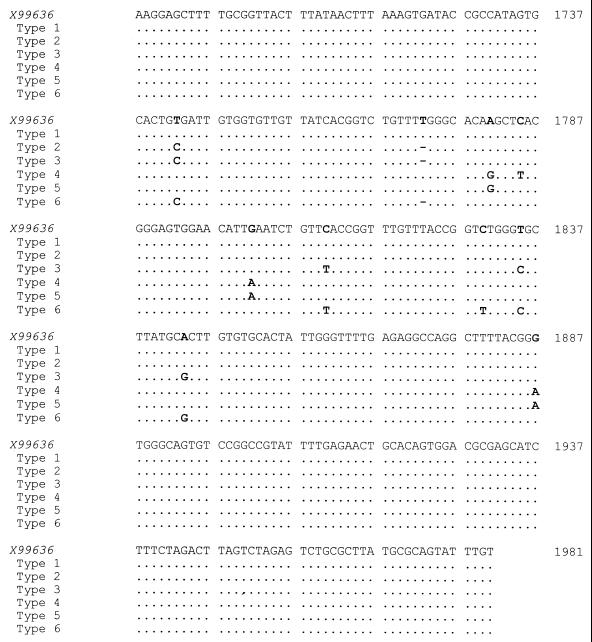
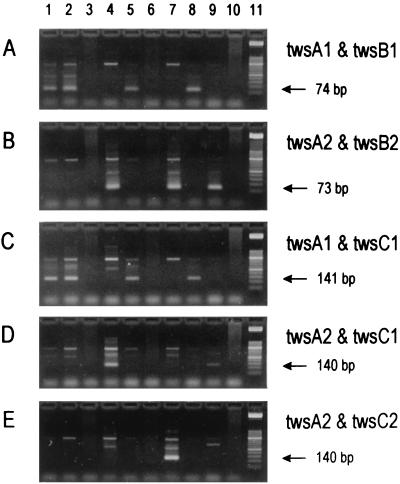
Whipple's disease is a rare bacterial infection that may involve any organ system in the body. It occurs primarily in Caucasian males older than 40 years. The gastrointestinal tract is the most frequently involved organ, with manifestations such as abdominal pain, malabsorption syndrome with diarrhea, and weight loss. Other signs include low-grade fever, lymphadenopathy, skin hyperpigmentation, endocarditis, pleuritis, seronegative arthritis, uveitis, spondylodiscitis, and neurological manifestations, and these signs may occur in the absence of gastrointestinal manifestations. Due to the wide variability of manifestations, clinical diagnosis is very difficult and is often made only years or even decades after the initial symptoms have appeared. Trimethoprim-sulfamethoxazole for at least 1 year is usually considered adequate to eradicate the infection. The microbiological diagnosis of this insidious disease is rendered difficult by the virtual lack of culture and serodiagnostic methods. It is usually based on the demonstration of periodic acid-Schiff-positive particles in infected tissues and/or the presence of bacteria with an unusual trilaminar cell wall ultrastructure by electron microscopy. Recently, the Whipple bacteria have been characterized at the molecular level by amplification of their 16S rRNA gene(s). Phylogenetic analysis of these sequences revealed a new bacterial species related to the actinomycete branch which was named "Tropheryma whippelli." Based on its unique 16S ribosomal DNA (rDNA) sequence, species-specific primers were selected for the detection of the organism in clinical specimens by PCR. This technique is currently used as one of the standard methods for establishing the diagnosis of Whipple's disease. Specific and broad-spectrum PCR amplifications mainly but not exclusively from extraintestinal specimens have significantly improved diagnosis, being more sensitive than histopathologic analysis. However, "T. whippelii" DNA has also been found in persons without clinical and histological evidence of Whipple's disease. It is unclear whether these patients are true asymptomatic carriers or whether differences in virulence exist among strains of "T. whippelii" that might account for the variable clinical manifestations. So far, six different "T. whippelii" subtypes have been found by analysis of their 16S-23S rDNA spacer region. Further studies of the pathogen "T. whippelii" as well as the host immune response are needed to fully understand this fascinating disease. The recent cultivation of the organisms is a promising major step in this direction.
Figures
Similar articles
-
Homogeneity of 16S-23S ribosomal intergenic spacer regions of Tropheryma whippelii in Swiss patients with Whipple's disease.J Clin Microbiol. 1999 Jan;37(1):152-6. doi: 10.1128/JCM.37.1.152-156.1999. J Clin Microbiol. 1999. PMID: 9854081 Free PMC article.
-
Evaluation of a specific nested PCR targeting domain III of the 23S rRNA gene of "Tropheryma whippelii" and proposal of a classification system for its molecular variants.J Clin Microbiol. 2000 Feb;38(2):595-9. doi: 10.1128/JCM.38.2.595-599.2000. J Clin Microbiol. 2000. PMID: 10655352 Free PMC article.
-
Whipple's disease and Tropheryma whippelii: secrets slowly revealed.Clin Infect Dis. 2001 Feb 1;32(3):457-63. doi: 10.1086/318512. Epub 2001 Jan 18. Clin Infect Dis. 2001. PMID: 11170954 Review.
-
Detection of three different types of 'Tropheryma whippelii' directly from clinical specimens by sequencing, single-strand conformation polymorphism (SSCP) analysis and type-specific PCR of their 16S-23S ribosomal intergenic spacer region.Int J Syst Bacteriol. 1999 Oct;49 Pt 4:1701-6. doi: 10.1099/00207713-49-4-1701. Int J Syst Bacteriol. 1999. PMID: 10555351
-
Whipple's disease.Dig Dis. 1995 Mar-Apr;13(2):108-18. doi: 10.1159/000171492. Dig Dis. 1995. PMID: 7586631 Review.
Cited by
-
Intrafamilial circulation of Tropheryma whipplei, France.Emerg Infect Dis. 2012 Jun;18(6):949-55. doi: 10.3201/eid1806.111038. Emerg Infect Dis. 2012. PMID: 22608161 Free PMC article.
-
Whipple's disease of the respiratory system: A case report.Exp Ther Med. 2024 Feb 7;27(4):133. doi: 10.3892/etm.2024.12421. eCollection 2024 Apr. Exp Ther Med. 2024. PMID: 38414785 Free PMC article.
-
Epidemiology of Whipple's Disease in the USA Between 2012 and 2017: A Population-Based National Study.Dig Dis Sci. 2019 May;64(5):1305-1311. doi: 10.1007/s10620-018-5393-9. Epub 2018 Nov 28. Dig Dis Sci. 2019. PMID: 30488239 Free PMC article.
-
Tropheryma whipplei Detection by Nanopore Sequencing in Patients With Interstitial Lung Disease.Front Microbiol. 2021 Nov 29;12:760696. doi: 10.3389/fmicb.2021.760696. eCollection 2021. Front Microbiol. 2021. PMID: 34912314 Free PMC article.
-
Tropheryma whipplei: a common bacterium in rural Senegal.PLoS Negl Trop Dis. 2011 Dec;5(12):e1403. doi: 10.1371/journal.pntd.0001403. Epub 2011 Dec 20. PLoS Negl Trop Dis. 2011. Retraction in: PLoS Negl Trop Dis. 2025 Jun 26;19(6):e0013229. doi: 10.1371/journal.pntd.0013229. PMID: 22206023 Free PMC article. Retracted.
References
-
- Adams M, Rhyner P A, Day J, DeArmond S, Smuckler E A. Whipple's disease confined to the central nervous system. Ann Neurol. 1987;21:104–108. - PubMed
-
- Adler C H, Galetta S L. Oculo-facial-skeletal myorhythmia in Whipple disease: treatment with ceftriaxone. Ann Intern Med. 1990;112:467–469. - PubMed
-
- Albrecht H, Rusch-Gerdes S, Stellbrink H J, Greten H, Jackle S. Disseminated Mycobacterium genavense infection as a cause of pseudo-Whipple's disease and sclerosing cholangitis. Clin Infect Dis. 1997;25:742–743. - PubMed
-
- Allchin W H, Hebb R G. Lymphangiectasis intestini. Trans Pathol Soc London. 1895;46:221–223.
-
- Altwegg M, Fleisch-Marx A, Goldenberger D, Hailemariam S, Schaffner A, Kissling R. Spondylodiscitis caused by Tropheryma whippelii. Schweiz Med Wochenschr. 1996;126:1495–1499. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
