

Referral for menstrual problems: cross sectional survey of symptoms, reasons for referral, and management
- PMID: 11440940
- PMCID: PMC34329
- DOI: 10.1136/bmj.323.7303.24
Referral for menstrual problems: cross sectional survey of symptoms, reasons for referral, and management
Abstract
Objectives: To describe the menstrual experience of women referred for menstrual problems, in particular menorrhagia (excessive menstrual loss), and to assess associations with reasons for referral given by their general practitioners, the women's understanding of the reasons for their attendance at the hospital clinics, and clinic outcome.
Design: Questionnaire survey, with partial review of case notes after 8 months.
Setting: Three hospital gynaecology clinics in Glasgow and Edinburgh.
Participants: 952 women completed the questionnaire, and the first 665 were reviewed.
Outcome measures: Reason for referral, women's reported menstrual problems and reason for clinic attendance, diagnosis, and treatment.
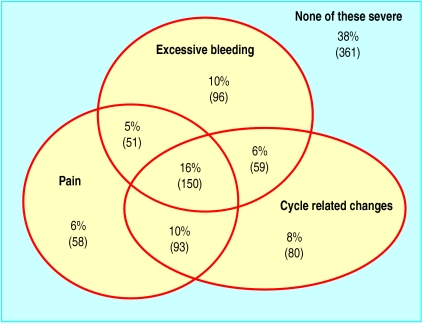
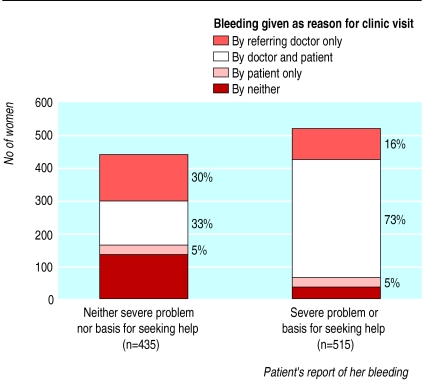
Results: Only 38% (95% confidence interval 34% to 41%) of women reported excessive menstrual loss as a severe problem. However 60% (57-63%) gave it as reason for attending a clinic, and 76% (73-79%) of general practitioners gave it as reason for referral. Reason for referral was significantly biased towards bleeding (McNemar odds ratio 4.01, 3.0 to 5.3, P<0.001) and against pain (0.54, 0.4 to 0.7, P<0.001). Dysfunctional uterine bleeding was diagnosed in 37% (31-42%) of the 259 women who gave as reason for attendance something other than bleeding. Women who were economically disadvantaged differed in prevalence of the main diagnoses and were more likely to fail to reattend. Hysterectomy was associated with referral for bleeding (relative risk 4.9, 1.6 to 15.6, P<0.001) but not with the patient stating bleeding as the reason for clinic attendance.
Conclusions: Intolerance of the volume of their bleeding is not a key feature among women attending clinics for bleeding problems. Broad menstrual complaint tends to be reframed as excessive bleeding at referral and during management. This may result in women receiving inappropriate care. Conceptualisation and assessment of menorrhagia requires reconsideration.
Figures

References
-
- Royal College of General Practitioners; Office of Population Censuses and Surveys; Department of Health. 1981-1982 Morbidity statistics from general practice. Third national study: socio-economic analysis, Series 5. London: HMSO; 1990.
-
- Bradlow J, Coulter A, Brooks P. Patterns of referral. Oxford: Oxford Health Services Research Unit; 1992.
-
- NHS Dissemination Centre. The management of menorrhagia. Effect Healthcare Bull 1995;9.
-
- Stirrat GM. Choice of treatment for menorrhagia. Lancet. 1999;353:2175–2176. - PubMed
-
- MORI. Women's health in 1990. Market Opinion and Research International; 1990. . (Research study conducted on behalf of Parke-Davis Laboratories.)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical