

Genioglossal inspiratory activation: central respiratory vs mechanoreceptive influences
- PMID: 11445198
- PMCID: PMC4372894
- DOI: 10.1016/s0034-5687(01)00230-4
Genioglossal inspiratory activation: central respiratory vs mechanoreceptive influences
Abstract
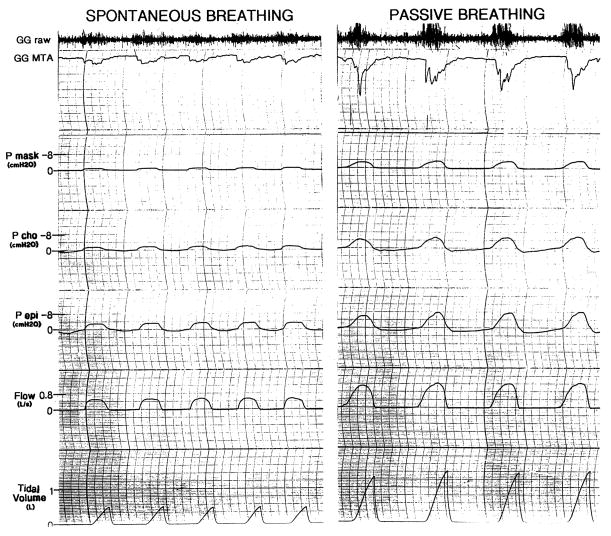
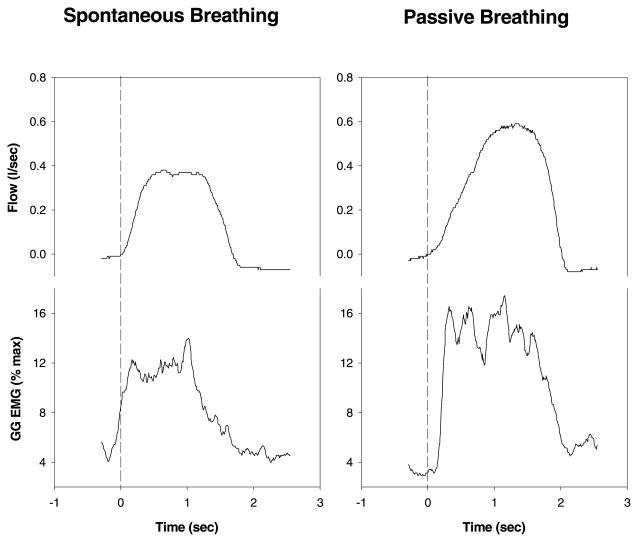
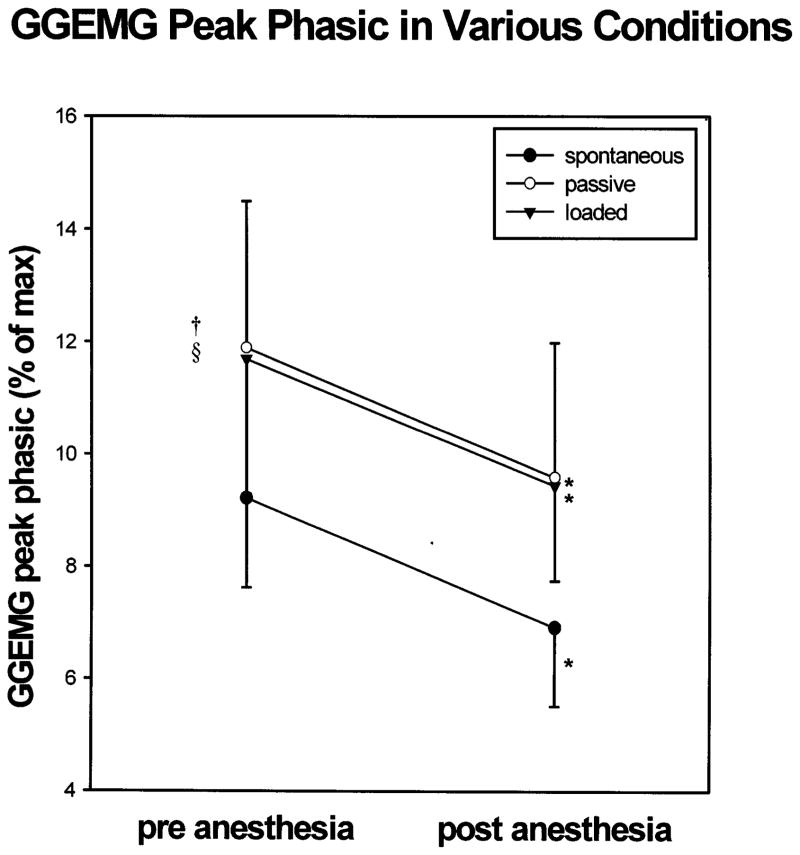
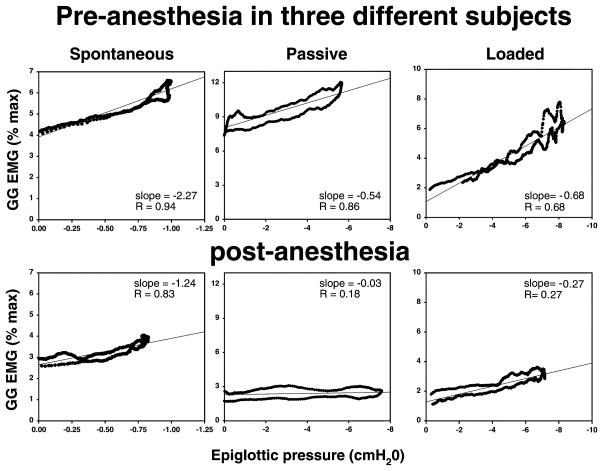
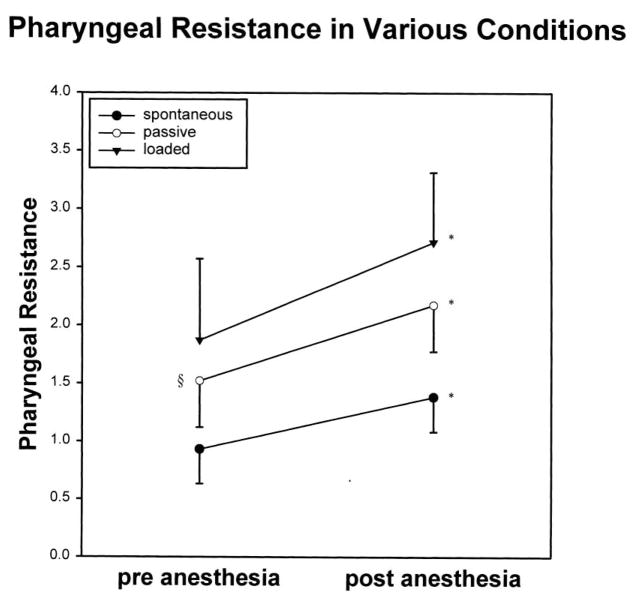
Upper airway dilator muscles are phasically activated during respiration. We assessed the interaction between central respiratory drive and local (mechanoreceptive) influences upon genioglossal (GG) activity throughout inspiration. GG(EMG) and airway mechanics were measured in 16 awake subjects during baseline spontaneous breathing, increased central respiratory drive (inspiratory resistive loading; IRL), and decreased respiratory drive (hypocapnic negative pressure ventilation), both prior to and following dense upper airway topical anesthesia. Negative epiglottic pressure (P(epi)) was significantly correlated with GG(EMG) across inspiration (i.e. within breaths). Both passive ventilation and IRL led to significant decreases in the sensitivity of the relationship between GG(EMG) and P(epi) (slope GG(EMG) vs P(epi)), but yielded no change in the relationship (correlation) between GG(EMG) and P(epi). During negative pressure ventilation, pharyngeal resistance increased modestly, but significantly. Anesthesia in all conditions led to decrements in phasic GG(EMG), increases in pharyngeal resistance, and decrease in the relationship between P(epi) and GG(EMG). We conclude that both central output to the GG and local reflex mediated activation are important in maintaining upper airway patency.
Figures
References
-
- Berry R, McNellis M, Kouchi K, Light R. Upper airway anesthesia reduces phasic genioglossus activity during sleep apnea. Am J Respir Crit Care Med. 1997;156:127–132. - PubMed
-
- Bianchi A, Denavit-Saubie M, Champagnat J. Central control of breathing in mammals: neuronal circuitry, membrane properties, and neurotransmitters. Physiol Rev. 1995;75:1–31. - PubMed
-
- Corfield D, Murphy K, Guz A. Does the motor cortical control of the diaphragm ‘bypass’ the brain stem respiratory centres in man? Respir Physiol. 1998;114:109–117. - PubMed
-
- Fogel R, Malhotra A, Edwards JK, Shea SA, White DP. Reduced genioglossal activity with upper airway anesthesia in awake patients with OSA. J Appl Physiol. 2000;88:1346–1354. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
