

Does tacrolimus offer virtual freedom from chronic rejection after primary liver transplantation? Risk and prognostic factors in 1,048 liver transplantations with a mean follow-up of 6 years
- PMID: 11460230
- PMCID: PMC2965463
- DOI: 10.1053/jlts.2001.25364
Does tacrolimus offer virtual freedom from chronic rejection after primary liver transplantation? Risk and prognostic factors in 1,048 liver transplantations with a mean follow-up of 6 years
Abstract
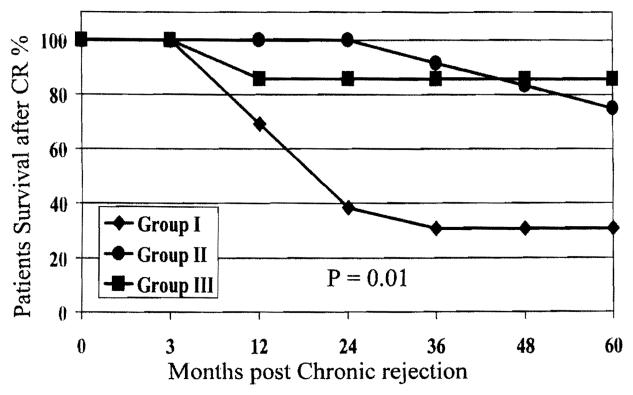
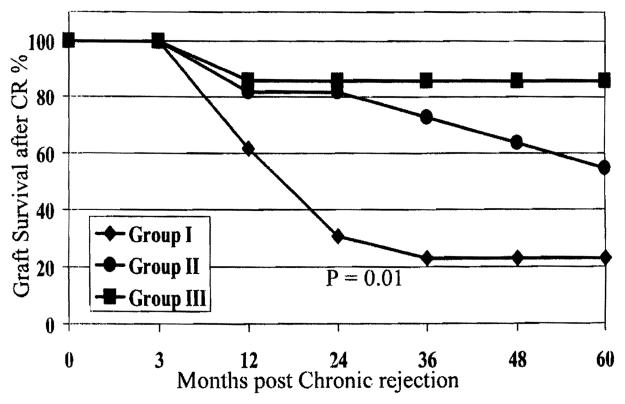
Tacrolimus has proven to be a potent immunosuppressive agent in liver transplantation (LT). Its introduction has led to significantly less frequent and severe acute rejection. Little is known about the rate of chronic rejection (CR) in primary LT using tacrolimus therapy. The aim of the present study is to examine the long-term incidence of CR, risk factors, prognostic factors, and outcome after CR. The present study evaluated the development of CR in 1,048 consecutive adult primary liver allograft recipients initiated and mostly maintained on tacrolimus-based immunosuppressive therapy. They were evaluated with a mean follow-up of 77.3 +/- 14.7 months (range, 50.7 to 100.1 months). To assess the impact of primary diagnosis on the rate and outcome of CR, the population was divided into 3 groups. Group I included patients with hepatitis C virus (HCV)- or hepatitis B virus (HBV)-induced cirrhosis (n = 312); group II included patients diagnosed with primary biliary cirrhosis (PBC), primary sclerosing cholangitis (PSC), or autoimmune hepatitis (AIH; n = 217); and group III included patients with all other diagnoses (n = 519). Overall, 32 of 1,048 patients (3.1%) developed CR. This represented 13 (4.1%), 12 (5.5%), and 7 patients (1.3%) in groups I, II, and III, respectively. The relative risk for developing CR was 3.2 times greater for group I and 4.3 times greater for group II compared with group III. This difference was statistically significant (P =.004). The incidence of acute rejection and total number of acute rejection episodes were significantly greater in patients who developed CR compared with those who did not (P <.0001). Similarly, the mean donor age for CR was significantly older than for patients without CR (43.0 v 36.2 years; P =.02). Thirteen of the 32 patients (40.6%) who developed CR retained their original grafts for a mean period of 54 +/- 25 months after diagnosis. Seven patients (21.9%) underwent re-LT, and 12 patients (38.3%) died. Serum bilirubin levels and the presence of arteriopathy, arterial loss, and duct loss on liver biopsy at the time of diagnosis of CR were significantly greater among the 3 groups of patients. In addition, patient and graft survival for group I were significantly worse compared with groups II and III. We conclude that CR occurred rarely among patients maintained long term on tacrolimus-based immunosuppressive therapy. When steroid use is controlled, the incidence of acute rejection, mean donor age, HBV- and/or HCV-induced cirrhosis, or a diagnosis of PBC, PSC, or AIH were found to be predictors of CR. Greater values for serum bilirubin level, duct loss, arteriopathy, arteriolar loss, and presence of HCV or HBV were found to be poor prognostic factors for the 3 groups; greater total serum bilirubin value (P =.05) was the only factor found to be significant between patients who had graft loss versus those who recovered.
Figures
Similar articles
-
The absence of chronic rejection in pediatric primary liver transplant patients who are maintained on tacrolimus-based immunosuppression: a long-term analysis.Transplantation. 2003 Apr 15;75(7):1020-5. doi: 10.1097/01.TP.0000056168.79903.20. Transplantation. 2003. PMID: 12698091
-
Early tacrolimus exposure after liver transplantation: relationship with moderate/severe acute rejection and long-term outcome.J Hepatol. 2013 Feb;58(2):262-70. doi: 10.1016/j.jhep.2012.09.019. Epub 2012 Sep 27. J Hepatol. 2013. PMID: 23023010
-
Incidence of rejection and infection after liver transplantation as a function of the primary disease: possible influence of alcohol and polyclonal immunoglobulins.Hepatology. 1996 Feb;23(2):240-8. doi: 10.1053/jhep.1996.v23.pm0008591847. Hepatology. 1996. PMID: 8591847
-
Tacrolimus: a further update of its use in the management of organ transplantation.Drugs. 2003;63(12):1247-97. doi: 10.2165/00003495-200363120-00006. Drugs. 2003. PMID: 12790696 Review.
-
Recurrent primary biliary cirrhosis, primary sclerosing cholangitis, and autoimmune hepatitis after transplantation.Semin Liver Dis. 2000;20(4):481-95. doi: 10.1055/s-2000-13157. Semin Liver Dis. 2000. PMID: 11200417 Review.
Cited by
-
Pediatric liver transplantation in 808 consecutive children: 20-years experience from a single center.Transplant Proc. 2002 Aug;34(5):1955-7. doi: 10.1016/s0041-1345(02)03136-6. Transplant Proc. 2002. PMID: 12176642 Free PMC article. No abstract available.
-
Liver transplantation.Gut Liver. 2009 Sep;3(3):145-65. doi: 10.5009/gnl.2009.3.3.145. Epub 2009 Sep 30. Gut Liver. 2009. PMID: 20431740 Free PMC article.
-
A network-based approach to identify expression modules underlying rejection in pediatric liver transplantation.Cell Rep Med. 2022 Apr 19;3(4):100605. doi: 10.1016/j.xcrm.2022.100605. eCollection 2022 Apr 19. Cell Rep Med. 2022. PMID: 35492246 Free PMC article.
-
Prognostic factors for the evolution and reversibility of chronic rejection in pediatric liver transplantation.Clinics (Sao Paulo). 2016 Apr;71(4):216-20. doi: 10.6061/clinics/2016(04)07. Clinics (Sao Paulo). 2016. PMID: 27166772 Free PMC article.
-
The effects of donor age on organ transplants: A review and implications for aging research.Exp Gerontol. 2018 Sep;110:230-240. doi: 10.1016/j.exger.2018.06.019. Epub 2018 Jun 20. Exp Gerontol. 2018. PMID: 29935294 Free PMC article. Review.
References
-
- Lowes JR, Hubscher SG, Neuberger JM. Chronic rejection of the liver allograft. Gastroenterol Clin North Am. 1993;22:401–420. - PubMed
-
- Hubscher SG, Buckels JA, Elias E, McMaster P, Neuberger J. Vanishing bile-duct syndrome following liver transplantation—Is it reversible? Transplantation. 1991;51:1004–1010. - PubMed
-
- Hayry P, Isoniemi H, Yilmaz S, Mennander A, Lemstrom K, Raisanen-Sokolowski A. Chronic allograft rejection. Immunol Rev. 1993;134:33–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical