

The evolution of methicillin-resistant Staphylococcus aureus in Canadian hospitals: 5 years of national surveillance
- PMID: 11468949
- PMCID: PMC81239
The evolution of methicillin-resistant Staphylococcus aureus in Canadian hospitals: 5 years of national surveillance
Abstract
Background: To better understand the epidemiology of methicillin-resistant Staphylococcus aureus (MRSA) in Canadian hospitals, surveillance has been conducted in sentinel hospitals across the country since 1995. We report the results of the first 5 years of the program.
Methods: For each newly identified inpatient with MRSA, medical records were reviewed for demographic and clinical data. Isolates were subjected to susceptibility testing and molecular typing by pulsed-field gel electrophoresis.
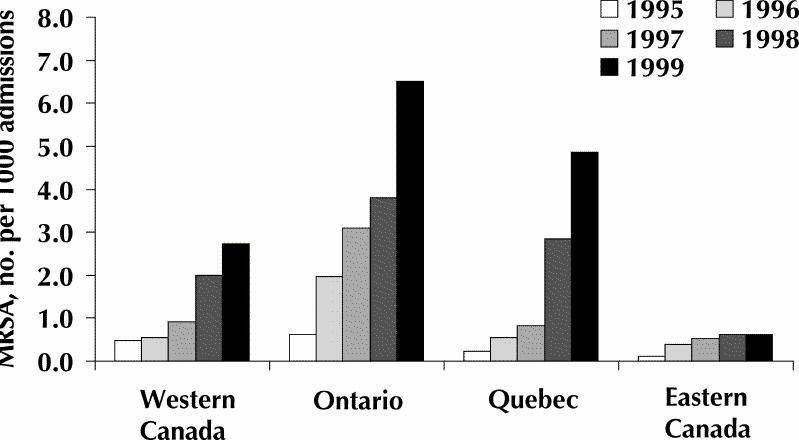
Results: A total of 4507 patients infected or colonized with MRSA were identified between January 1995 and December 1999. The rate of MRSA increased each year from a mean of 0.95 per 100 S. aureus isolates in 1995 to 5.97 per 100 isolates in 1999 (0.46 per 1000 admissions in 1995 to 4.12 per 1000 admissions in 1999) (p < 0.05). Most of the increase in MRSA occurred in Ontario, Quebec and the western provinces. Of the 3009 cases for which the site of MRSA acquisition could be determined, 86% were acquired in a hospital, 8% were acquired in a long-term care facility and 6% were acquired in the community. A total of 1603 patients (36%) were infected with MRSA. The most common sites of infection were skin or soft tissue (25% of MRSA infections), pulmonary tissues (24%) and surgical sites (23%); 13% of the patients were bacteremic. An epidemiologic link with a previously identified MRSA patient was suspected in 53% of the cases. Molecular typing indicated that most (81%) of the isolates could be classified as related to 1 of the 4 Canadian epidemic strains of MRSA.
Interpretation: There has been a significant increase in the rate of isolating MRSA in many Canadian hospitals, related to the transmission of a relatively small number of MRSA strains.
Figures
Comment in
-
Stopping short the spread of methicillin-resistant Staphylococcus aureus.CMAJ. 2001 Jul 10;165(1):31-2. CMAJ. 2001. PMID: 11468951 Free PMC article. No abstract available.
Similar articles
-
Mupirocin-resistant, methicillin-resistant Staphylococcus aureus strains in Canadian hospitals.Antimicrob Agents Chemother. 2007 Nov;51(11):3880-6. doi: 10.1128/AAC.00846-07. Epub 2007 Aug 27. Antimicrob Agents Chemother. 2007. PMID: 17724154 Free PMC article.
-
Methicillin-resistant Staphylococcus aureus colonization or infection in Canada: National Surveillance and Changing Epidemiology, 1995-2007.Infect Control Hosp Epidemiol. 2010 Apr;31(4):348-56. doi: 10.1086/651313. Infect Control Hosp Epidemiol. 2010. PMID: 20148693
-
Three-year surveillance of community onset health care-associated staphylococcus aureus infections in children.Pediatr Infect Dis J. 2006 Apr;25(4):349-53. doi: 10.1097/01.inf.0000207404.50143.1e. Pediatr Infect Dis J. 2006. PMID: 16567988
-
National surveillance of methicillin-resistant Staphylococcus aureus among hospitalized pediatric patients in Canadian acute care facilities, 1995-2007.Pediatr Infect Dis J. 2012 Aug;31(8):814-20. doi: 10.1097/INF.0b013e31825c48a0. Pediatr Infect Dis J. 2012. PMID: 22565289
-
Laboratory and epidemiologic experience with methicillin-resistant Staphylococcus aureus in the USA.Eur J Clin Microbiol. 1986 Dec;5(6):693-6. doi: 10.1007/BF02013307. Eur J Clin Microbiol. 1986. PMID: 3542532 Review.
Cited by
-
Rapid detection of methicillin-resistant staphylococci from blood culture bottles by using a multiplex PCR assay.J Clin Microbiol. 2002 Aug;40(8):2786-90. doi: 10.1128/JCM.40.8.2786-2790.2002. J Clin Microbiol. 2002. PMID: 12149330 Free PMC article.
-
Occurrence of antimicrobial resistant bacteria in healthy dogs and cats presented to private veterinary hospitals in southern Ontario: A preliminary study.Can Vet J. 2009 Oct;50(10):1047-53. Can Vet J. 2009. PMID: 20046603 Free PMC article.
-
Nationwide trends in molecular epidemiology of methicillin-resistant Staphylococcus aureus, Finland, 1997-2004.BMC Infect Dis. 2007 Aug 14;7:94. doi: 10.1186/1471-2334-7-94. BMC Infect Dis. 2007. PMID: 17697340 Free PMC article.
-
Clinical practice guidelines for hospital-acquired pneumonia and ventilator-associated pneumonia in adults.Can J Infect Dis Med Microbiol. 2008 Jan;19(1):19-53. doi: 10.1155/2008/593289. Can J Infect Dis Med Microbiol. 2008. PMID: 19145262 Free PMC article.
-
Comparative genomics of Canadian epidemic lineages of methicillin-resistant Staphylococcus aureus.J Clin Microbiol. 2007 Jun;45(6):1904-11. doi: 10.1128/JCM.02500-06. Epub 2007 Apr 11. J Clin Microbiol. 2007. PMID: 17428941 Free PMC article.
References
-
- Townsend DE, Ashdown N, Bolton S, Bradley J, Duckworth G, Moorhouse EC, et al. The international spread of methicillin-resistant Staphylococcus aureus. J Hosp Infect 1987;9:60-71. - PubMed
-
- Panlilio AL, Culver DH, Gaynes RP, Banerjee S, Henderson TS, Tolson JS, et al, and the National Nosocomial Infections Surveillance System. Methicillin-resistant Staphylococcus aureus in U.S. hospitals, 1975–1991. Infect Control Hosp Epidemiol 1992;13:582-6. - PubMed
-
- Voss A, Milatovic D, Wallrauch-Schwarz C, Rosdahl VT, Braveny I. Methicillin-resistant Staphylococcus aureus in Europe. Eur J Clin Microbiol Infect Dis 1994; 13:50-5. - PubMed
-
- Riley TV, Pearman JW, Rouse IL. Changing epidemiology of methicillin-resistant Staphylococcus aureus in Western Australia. Med J Aust 1995;163:412-4. - PubMed
-
- Cox RA, Conquest C, Mallaghan C, Marples RR. A major outbreak of methicillin-resistant Staphylococcus aureus caused by a new phage-type (EMRSA-16). J Hosp Infect 1995;29:87-106. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical