

Improved antimicrobial interventions have benefits
- PMID: 11473998
- PMCID: PMC88245
- DOI: 10.1128/JCM.39.8.2823-2828.2001
Improved antimicrobial interventions have benefits
Abstract
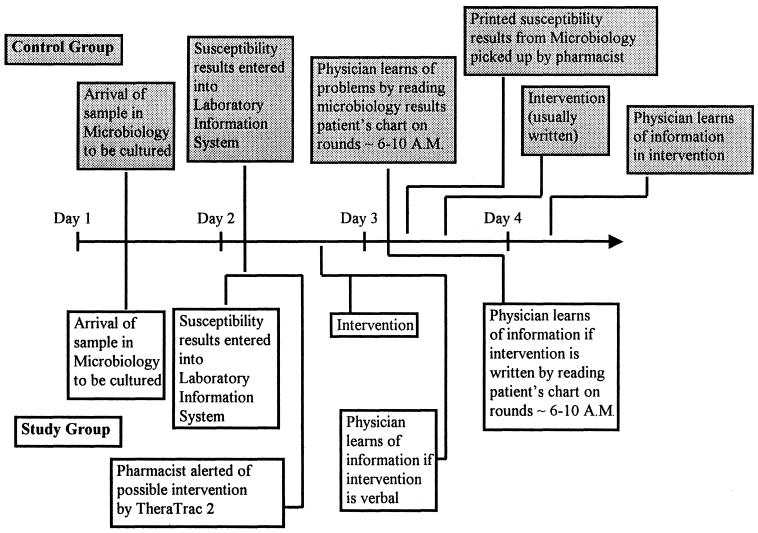
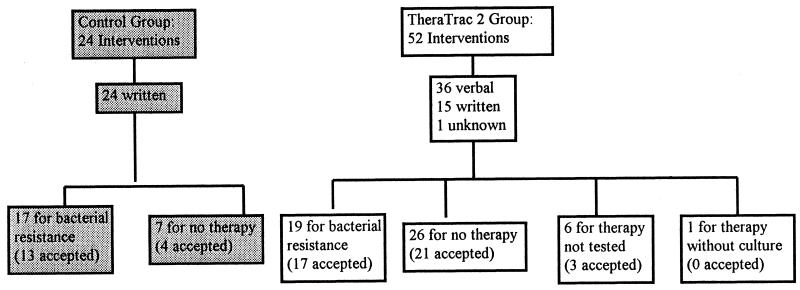
Studies have shown benefits to patients from improved interventions involving antimicrobial therapy. The purpose of the present study was to evaluate prospectively the impact of improved interventions by (i) the use of TheraTrac 2, a computer software program which electronically links susceptibility testing results immediately to the pharmacy and alerts pharmacists of potential interventions, and (ii) the education of pharmacists involving microbiologic topics. The study group had the new intervention program. The control group had interventions performed the way that they had previously been done by manually reviewing hard copies of susceptibility testing data. In a 5-month period, all inpatients whose last names began with A to K were the study group; inpatients whose last names began with L to Z were controls. Three analyses were done; one analysis (analysis A) involved only patients with interventions, one analysis (analysis B) involved all patients for whom antimicrobial testing was done and who were matched for diagnosis-related groups (DRGs), regardless of whether an intervention occurred, and one analysis (analysis C) involved these DRG-matched patients by using severity-adjusted data. In analysis A, the study group had a 4.8% decreased rate of mortality, an average of a 16.5-day decreased length of stay per patient, and $20,886 decreased variable direct costs per patient. None of these differences was statistically significant. In analysis B, the study patients had a 1.2% higher mortality rate (P = 0.741), an average of a 2.7-day decreased length of stay per patient (P = 0.035), and $2,626 decreased variable direct costs per patient (P = 0.008). In analysis C, the study patients had a 1.4% lower mortality rate, a 1.2-day decreased length of stay per patient, and $1,466 decreased variable direct costs per patient. In conclusion, the institution of this program caused substantial cost savings.
Figures
References
-
- Dawson (-Saunders) B, Trapp R. Biostatistics. 2nd ed. Norwalk, Conn: Appleton and Lange; 1994.
-
- Evans R S, Klassen D C, Pestotnik S L, et al. Improving empiric antibiotic selection using computer decision support. Arch Intern Med. 1994;54:878–884. - PubMed
-
- Evans R S, Pestotnik F L, Klassen D C, et al. Computer-assisted management program for antibiotics and other antiinfective agents. N Engl J Med. 1998;338:232–238. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
