

Assessment, by transcription-mediated amplification, of virologic response in patients with chronic hepatitis C virus treated with peginterferon alpha-2a
- PMID: 11474002
- PMCID: PMC88249
- DOI: 10.1128/JCM.39.8.2850-2855.2001
Assessment, by transcription-mediated amplification, of virologic response in patients with chronic hepatitis C virus treated with peginterferon alpha-2a
Abstract
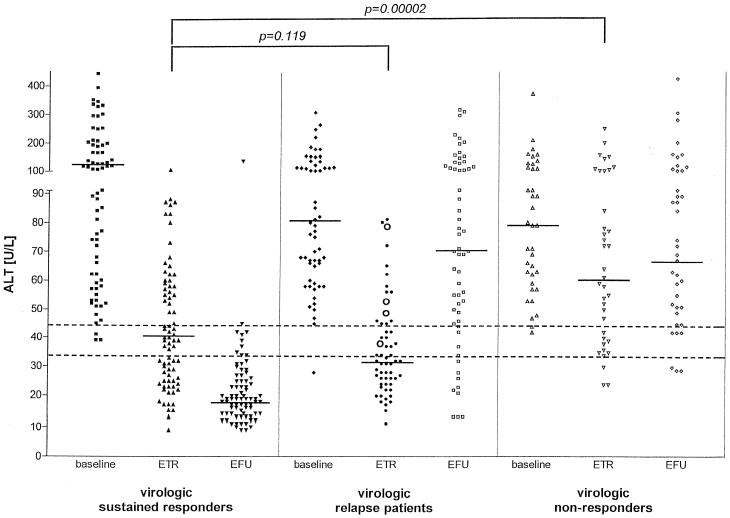
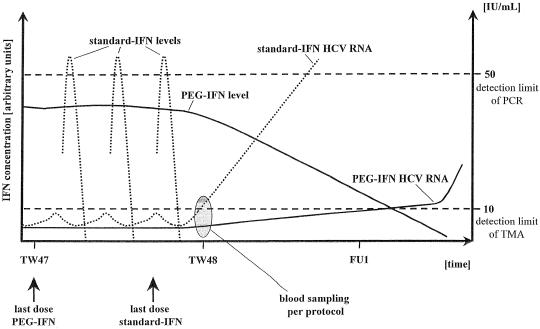
Transcription-mediated amplification (TMA) is an isothermal, autocatalytic target amplification method which has the potential to detect less than 50 hepatitis C virus (HCV) RNA copies/ml (10 IU/ml). The TMA assay was used to assess the presence of residual HCV RNA in plasma from patients treated with polyethylene glycol-modified interferon alpha-2a (peginterferon alpha-2a) who showed a virologic relapse after the end of therapy. Stored end-of-treatment and end-of-follow-up plasma samples from 177 of 267 patients treated with peginterferon alpha-2a (S. Zeuzem et al., N. Engl. J. Med. 343:1666--1672, 2000) were available for retesting by TMA. Plasma samples from patients in the same study who exhibited virologic relapse after treatment with standard interferon alpha-2a served as controls. Virologic response during the trial was defined as HCV RNA that was undetectable using a PCR-based test system with a sensitivity of 50 IU/mL (Cobas Amplicor HCV version 2.0) and was compared with TMA-based retesting results (VERSANT HCV RNA Qualitative Assay). Residual HCV RNA was detected in 4 of 60 cases (7%) by the TMA technology in end-of-treatment plasma samples from patients who relapsed after receiving peginterferon alpha-2a and in 6 of 18 patients (33%) following therapy with standard interferon alpha-2a. For peginterferon alpha-2a-treated patients with sustained virologic response, HCV RNA was detectable by TMA in end-of-treatment samples in 3 of 78 cases but in none of the end-of-follow-up samples. For all end-of-treatment and end-of-follow-up plasma samples of virologic nonresponders, a complete concordance between the PCR-based assay and TMA was observed. In conclusion, in patients with virologic relapse after the end of therapy, according to PCR, who were treated with peginterferon alpha-2a or standard interferon alpha-2a, residual HCV RNA was detectable in end-of-treatment samples by the TMA-based assay in 7 or 33% of cases, respectively. The lower rate of residual HCV RNA detection by TMA for patients treated with peginterferon alpha-2a than that for patients treated with standard interferon alpha-2a may be due to the maintained antiviral pressure of the long-acting peginterferon alpha-2a at the end-of-treatment visit.
Figures
References
-
- Algranati N E, Sy S, Modi M. A branched methoxy 40 kDa polyethylene glycol (PEG) moiety optimizes the pharmacokinetics (PK) of peginterferon alfa-2a (PEG-IFN) and may explain its enhanced efficacy in chronic hepatitis C (CHC) Hepatology. 1999;30(Suppl. 4):190A.
-
- Alter M J, Margolis H S, Krawczynski K, Judson F N, Mares A, Alexander W J, Hu P Y, Miller J K, Gerber M A, Sampliner R E, et al. The natural history of community-acquired hepatitis C in the United States. The Sentinel Counties Chronic non-A, non-B Hepatitis Study Team. N Engl J Med. 1992;327:1899–1905. - PubMed
-
- Carithers R L, Jr, Emerson S S. Therapy of hepatitis C: meta-analysis of interferon alfa-2b trials. Hepatology. 1997;26(Suppl. 1):83S–88S. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
