

Dumbbell schwannomas of the internal auditory canal
- PMID: 11498429
- PMCID: PMC7975197
Dumbbell schwannomas of the internal auditory canal
Abstract
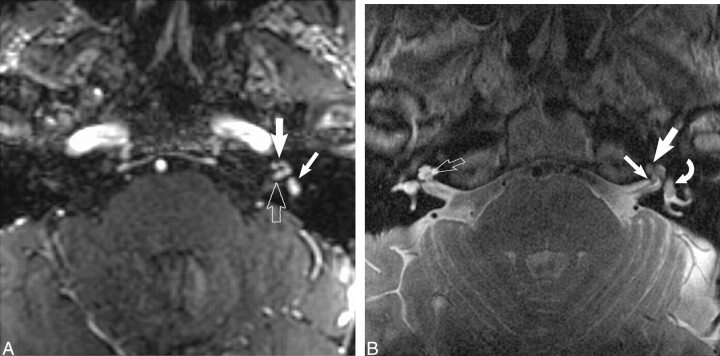
Background and purpose: Benign tumors of the internal auditory canal (IAC) may leave the confines of the IAC fundus and extend into inner ear structures, forming a dumbbell-shaped lesion. It is important to differentiate dumbbell lesions, which include facial and vestibulocochlear schwannomas, from simple intracanalicular schwannomas, as surgical techniques and prognostic implications are affected. In this article, the imaging and clinical features of these dumbbell schwannomas are described.
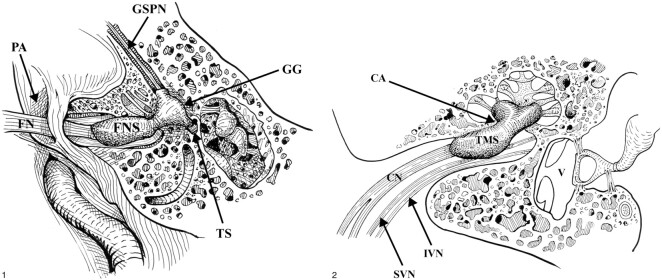
Methods: A dumbbell lesion of the IAC is defined as a mass with two bulbous segments, one in the IAC fundus and the other in the membranous labyrinth of the inner ear or the geniculate ganglion of the facial nerve canal, spanned by an isthmus. Twenty-four patients with dumbbell lesions of the IAC had their clinical and imaging data retrospectively reviewed. Images were evaluated for contour of the mass and extension into the membranous labyrinth or geniculate ganglion.
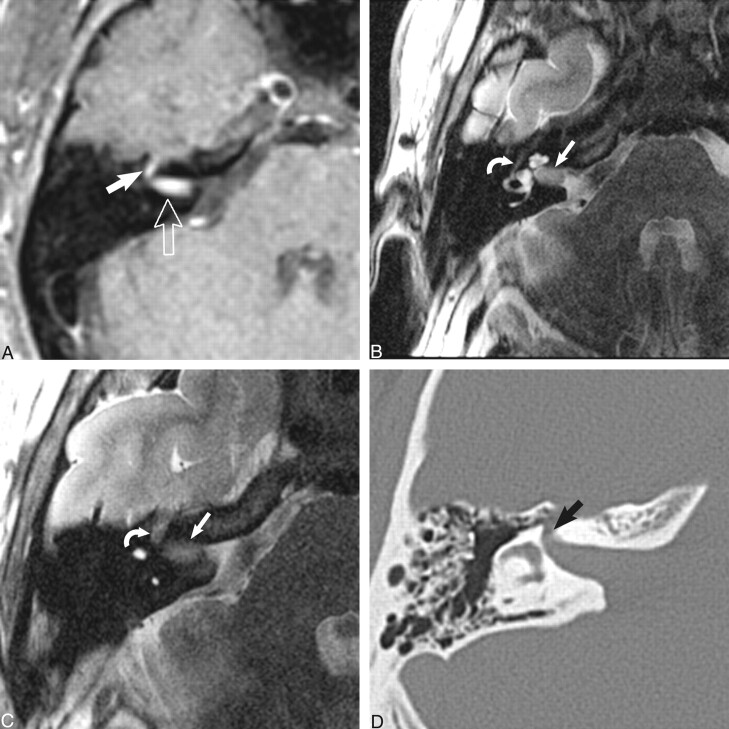
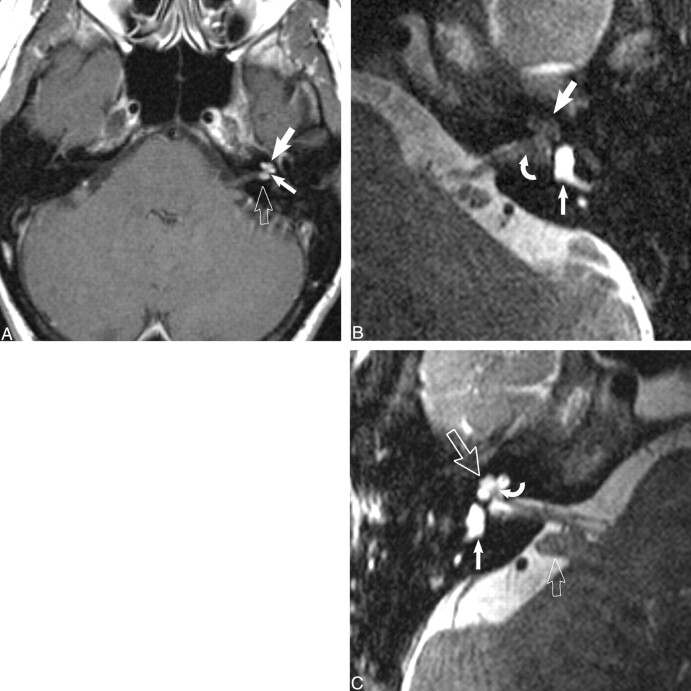
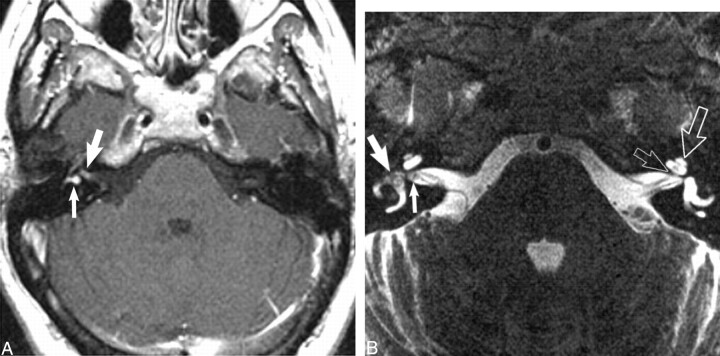
Results: Ten of 24 lesions were facial nerve dumbbell lesions. Characteristic features included an enhancing "tail" along the labyrinthine segment of the facial nerve and enlargement of the facial nerve canal. Dumbbell schwannomas of the vestibulocochlear nerve (14/24) included transmodiolar (8/14), which extended into the cochlea, transmacular (2/14), which extended into the vestibule, and combined transmodiolar/transmacular (4/14) types.
Conclusion: Simple intracanalicular schwannomas can be differentiated from transmodiolar, transmacular, and facial nerve schwannomas with postcontrast and high-resolution fast spin-echo T2-weighted MR imaging. Temporal bone CT is reserved for presurgical planning in the dumbbell facial nerve schwannoma group.
Figures

Similar articles
-
MRI of inner ear and facial nerve pathology using 3D MP-RAGE and 3D CISS sequences.Br J Radiol. 1997 Jun;70(834):558-66. doi: 10.1259/bjr.70.834.9227246. Br J Radiol. 1997. PMID: 9227246 Clinical Trial.
-
Dural tail: another face of facial nerve schwannoma?AJNR Am J Neuroradiol. 2006 Oct;27(9):1804; author reply 1805. AJNR Am J Neuroradiol. 2006. PMID: 17032843 Free PMC article. No abstract available.
-
The vestibulocochlear nerve (VIII).Diagn Interv Imaging. 2013 Oct;94(10):1043-50. doi: 10.1016/j.diii.2013.08.015. Epub 2013 Oct 1. Diagn Interv Imaging. 2013. PMID: 24095603 Review.
-
[Facial nerve schwannoma in the inner auditory canal and geniculate ganglion].HNO. 2003 Aug;51(8):640-5. doi: 10.1007/s00106-002-0788-4. Epub 2003 Apr 4. HNO. 2003. PMID: 12942179 German.
-
Stenosis of the internal auditory meatus masquerading as bilateral vestibular schwannomas: a cautionary tale.J Laryngol Otol. 2005 Dec;119(12):995-7. doi: 10.1258/002221505775010689. J Laryngol Otol. 2005. PMID: 16354367 Review.
Cited by
-
Complete resection versus functional preservation in resection of cystic vestibular schwannoma in a 56-year-old female: case report and literature review.J Surg Case Rep. 2023 Dec 14;2023(12):rjad655. doi: 10.1093/jscr/rjad655. eCollection 2023 Dec. J Surg Case Rep. 2023. PMID: 38111494 Free PMC article.
-
Imaging of cerebellopontine angle lesions: an update. Part 1: enhancing extra-axial lesions.Eur Radiol. 2007 Oct;17(10):2472-82. doi: 10.1007/s00330-007-0679-x. Epub 2007 Jun 12. Eur Radiol. 2007. PMID: 17562049 Review.
-
Imaging of sensorineural hearing loss: a pattern-based approach to diseases of the inner ear and cerebellopontine angle.Insights Imaging. 2012 Apr;3(2):139-53. doi: 10.1007/s13244-011-0134-z. Epub 2011 Dec 9. Insights Imaging. 2012. PMID: 22696040 Free PMC article.
-
Mass screening for retrocochlear disorders: low-field-strength (0.2-T) versus high-field-strength (1.5-T) MR imaging.AJNR Am J Neuroradiol. 2002 Jun-Jul;23(6):918-23. AJNR Am J Neuroradiol. 2002. PMID: 12063216 Free PMC article. Clinical Trial.
-
Auditory Pathway Features Determined by DTI in Subjects with Unilateral Acoustic Neuroma.Clin Neuroradiol. 2016 Dec;26(4):439-444. doi: 10.1007/s00062-015-0385-z. Epub 2015 Mar 27. Clin Neuroradiol. 2016. PMID: 25813527
References
-
- Swartz JD, Harnsberger HR. Imaging of the Temporal Bone. 3rd ed. New York: Thieme;1998:370–435
-
- Hasso AN, Smith DS. The cerebellopontine angle. Semin Ultrasound CT MR 1989;10:280-301 - PubMed
-
- Clemis JD, Ballad WJ, Baggot PJ, Lyon ST. Relative frequency of the inferior vestibular schwannoma. Arch Otolaryngol Head Neck Surg 1986;112:190-194 - PubMed
-
- Green JD Jr, McKenzie JD. Diagnosis and management of intralabyrinthine schwannomas. Laryngoscope 1999;109:1626-1631 - PubMed
-
- Schunknecht HF. Pathology of the Ear. 2nd ed. Malvern, PA: Lea and Febiger;1993:460–474
MeSH terms
LinkOut - more resources
Full Text Sources
Medical