

T-cell reactivity against streptococcal antigens in the periphery mirrors reactivity of heart-infiltrating T lymphocytes in rheumatic heart disease patients
- PMID: 11500404
- PMCID: PMC98644
- DOI: 10.1128/IAI.69.9.5345-5351.2001
T-cell reactivity against streptococcal antigens in the periphery mirrors reactivity of heart-infiltrating T lymphocytes in rheumatic heart disease patients
Abstract
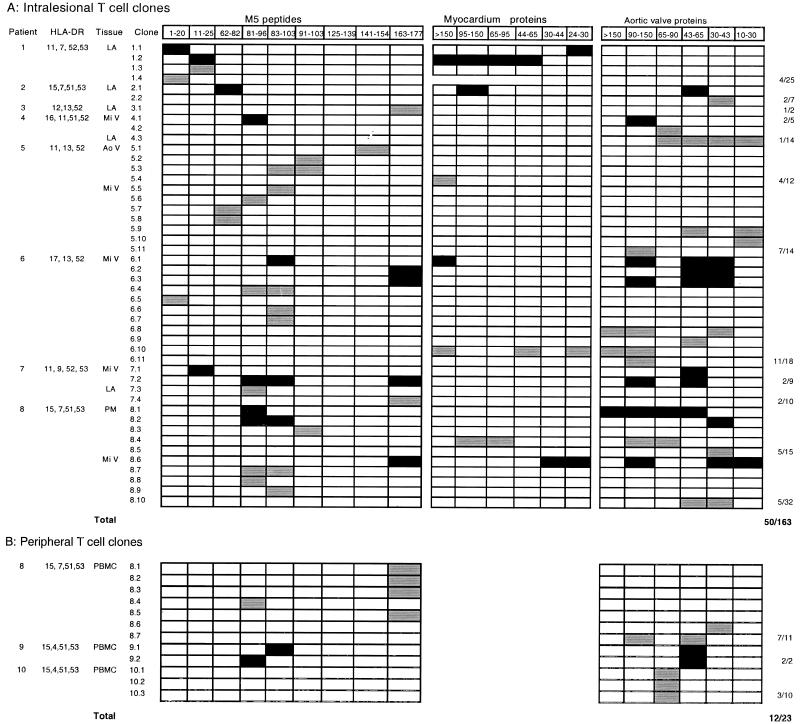
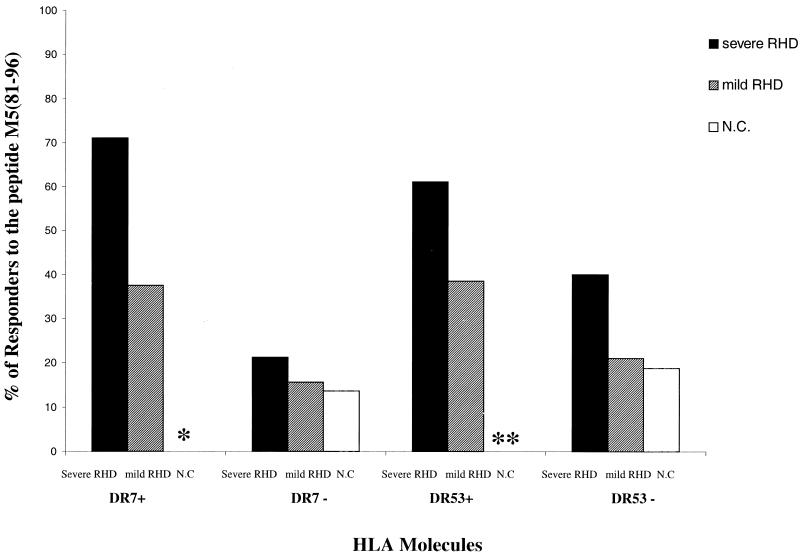
T-cell molecular mimicry between streptococcal and heart proteins has been proposed as the triggering factor leading to autoimmunity in rheumatic heart disease (RHD). We searched for immunodominant T-cell M5 epitopes among RHD patients with defined clinical outcomes and compared the T-cell reactivities of peripheral blood and intralesional T cells from patients with severe RHD. The role of HLA class II molecules in the presentation of M5 peptides was also evaluated. We studied the T-cell reactivity against M5 peptides and heart proteins on peripheral blood mononuclear cells (PBMC) from 74 RHD patients grouped according to the severity of disease, along with intralesional and peripheral T-cell clones from RHD patients. Peptides encompassing residues 1 to 25, 81 to 103, 125 to 139, and 163 to 177 were more frequently recognized by PBMC from RHD patients than by those from controls. The M5 peptide encompassing residues 81 to 96 [M5(81-96) peptide] was most frequently recognized by PBMC from HLA-DR7+ DR53+ patients with severe RHD, and 46.9% (15 of 32) and 43% (3 of 7) of heart-infiltrating and PBMC-derived peptide-reactive T-cell clones, respectively, recognized the M5(81-103) region. Heart proteins were recognized more frequently by PBMC from patients with severe RHD than by those from patients with mild RHD. The similar pattern of T-cell reactivity found with both peripheral blood and heart-infiltrating T cells is consistent with the migration of M-protein-sensitized T cells to the heart tissue. Conversely, the presence of heart-reactive T cells in the PBMC of patients with severe RHD also suggests a spillover of sensitized T cells from the heart lesion.
Figures
Similar articles
-
Rheumatic fever: how S. pyogenes-primed peripheral T cells trigger heart valve lesions.Ann N Y Acad Sci. 2005 Jun;1051:132-40. doi: 10.1196/annals.1361.054. Ann N Y Acad Sci. 2005. PMID: 16126952 Review.
-
How an autoimmune reaction triggered by molecular mimicry between streptococcal M protein and cardiac tissue proteins leads to heart lesions in rheumatic heart disease.J Autoimmun. 2005 Mar;24(2):101-9. doi: 10.1016/j.jaut.2005.01.007. J Autoimmun. 2005. PMID: 15829402
-
T cell response in rheumatic fever: crossreactivity between streptococcal M protein peptides and heart tissue proteins.Curr Protein Pept Sci. 2007 Feb;8(1):39-44. doi: 10.2174/138920307779941488. Curr Protein Pept Sci. 2007. PMID: 17305559 Review.
-
Rheumatic fever: the T cell response leading to autoimmune aggression in the heart.Autoimmun Rev. 2002 Oct;1(5):261-6. doi: 10.1016/s1568-9972(02)00062-9. Autoimmun Rev. 2002. PMID: 12848978 Review.
-
Mimicry in recognition of cardiac myosin peptides by heart-intralesional T cell clones from rheumatic heart disease.J Immunol. 2006 May 1;176(9):5662-70. doi: 10.4049/jimmunol.176.9.5662. J Immunol. 2006. PMID: 16622036
Cited by
-
Rheumatic Fever.Images Paediatr Cardiol. 2002 Apr;4(2):12-31. Images Paediatr Cardiol. 2002. PMID: 22368613 Free PMC article.
-
Rheumatic heart disease: proinflammatory cytokines play a role in the progression and maintenance of valvular lesions.Am J Pathol. 2004 Nov;165(5):1583-91. doi: 10.1016/S0002-9440(10)63415-3. Am J Pathol. 2004. PMID: 15509528 Free PMC article.
-
Rheumatic Heart Disease: Molecules Involved in Valve Tissue Inflammation Leading to the Autoimmune Process and Anti-S. pyogenes Vaccine.Front Immunol. 2013 Oct 30;4:352. doi: 10.3389/fimmu.2013.00352. Front Immunol. 2013. PMID: 24198818 Free PMC article. Review.
-
Anti-group A streptococcal vaccine epitope: structure, stability, and its ability to interact with HLA class II molecules.J Biol Chem. 2011 Mar 4;286(9):6989-98. doi: 10.1074/jbc.M110.132118. Epub 2010 Dec 17. J Biol Chem. 2011. PMID: 21169359 Free PMC article.
-
In silico prediction of peptides binding to multiple HLA-DR molecules accurately identifies immunodominant epitopes from gp43 of Paracoccidioides brasiliensis frequently recognized in primary peripheral blood mononuclear cell responses from sensitized individuals.Mol Med. 2003 Sep-Dec;9(9-12):209-19. Mol Med. 2003. PMID: 15208742 Free PMC article.
References
-
- Anastasiou-Nana M, Anderson J L, Carlquist J F, Nana J N. HLA DR typing and lymphocyte subset evaluation in rheumatic heart disease: a search for immune response factors. Am Heart J. 1986;112:992–997. - PubMed
-
- Bromelow K V, Souberbielle B, Alavi A, Goldman J H, Libera L D, Dalgleish A G, McKenna W J. Lack of T cell response to cardiac myosin and a reduced response to PPD in patients with idiopathic dilated cardiomyopathy. J Autoimmun. 1997;10:219–227. - PubMed
-
- Dajani A S, Ayoub E, Bierman F Z, Bisno A L, Deny F W, Durack D T, Ferrieri P, Freed M, Gerber M, Kaplan E L, Karchmer A W, Markowitz M, Rahimtoola, Shulman S, Stollerman G, Takahashi M, Taranta A, Taubert K A, Wilson W. Guidelines for diagnosis of rheumatic fever: Jones criteria, updated 1992. Circulation. 1993;87:302–307.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
