

2,500 living donor kidney transplants: a single-center experience
- PMID: 11505060
- PMCID: PMC1422001
- DOI: 10.1097/00000658-200108000-00004
2,500 living donor kidney transplants: a single-center experience
Abstract
Objective: To review a single center's experience and outcome with living donor transplants.
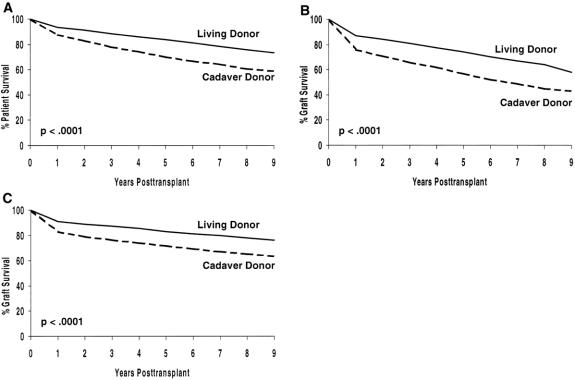
Summary background data: Outcome after living donor transplants is better than after cadaver donor transplants. Since the inception of the authors' program, they have performed 2,540 living donor transplants. For the most recent cohort of recipients, improvements in patient care and immunosuppressive protocols have improved outcome. In this review, the authors analyzed outcome in relation to protocol.
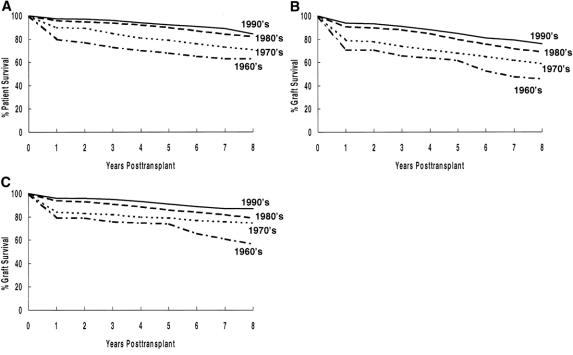
Methods: The authors studied patient and graft survival by decade. For those transplanted in the 1990s, the impact of immunosuppressive protocol, donor source, diabetes, and preemptive transplantation was analyzed. The incidence of rejection, posttransplant steroid-related complications, and return to work was determined. Finally, multivariate analysis was used to study risk factors for worse 1-year graft survival and, for those with graft function at 1 year, to study risk factors for worse long-term survival.
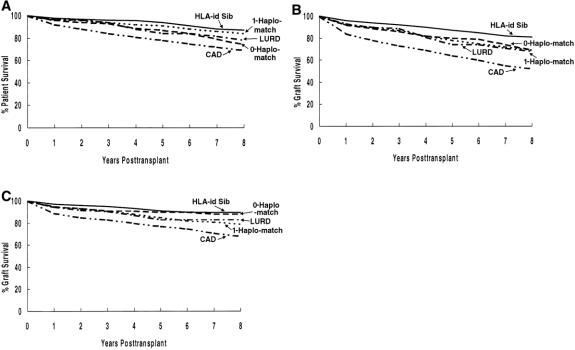
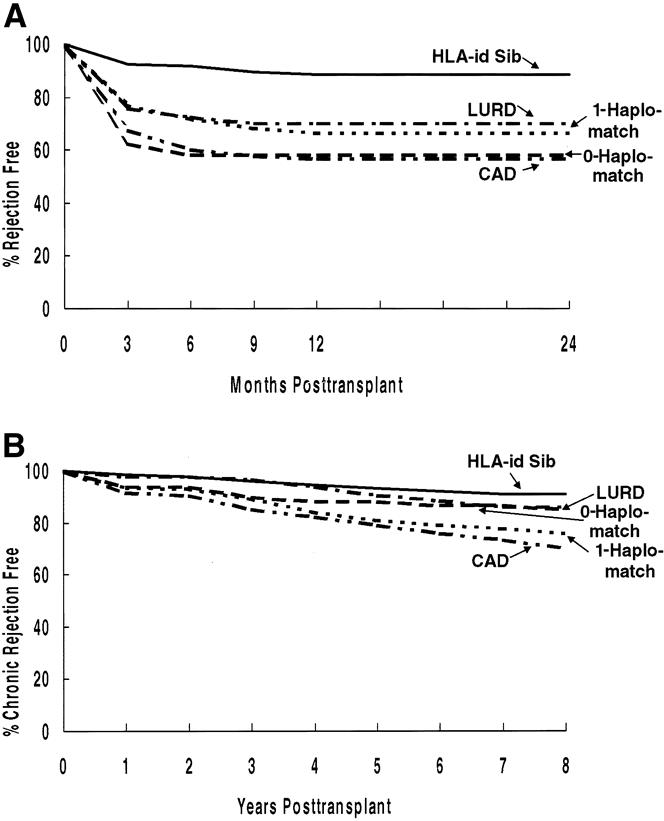
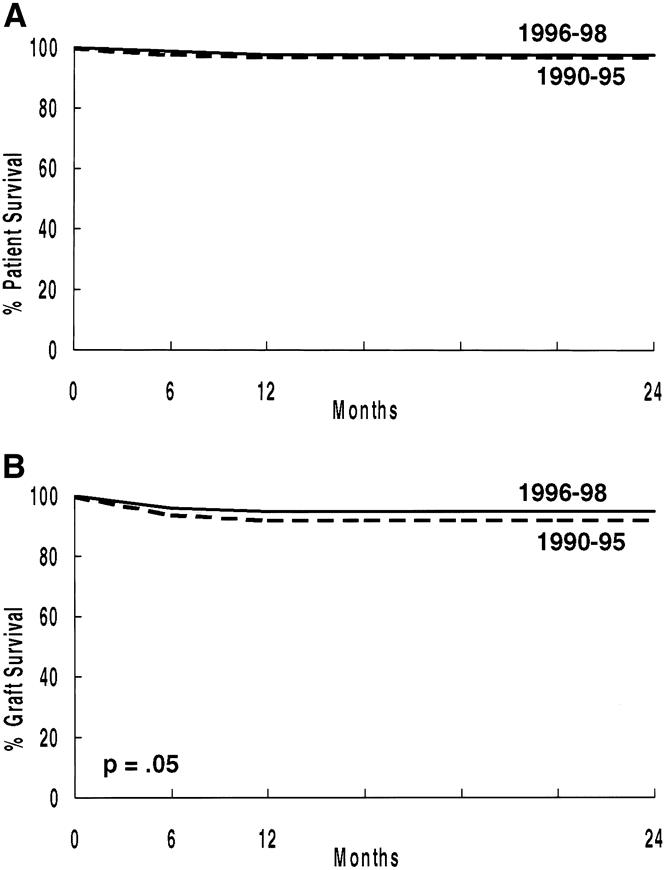
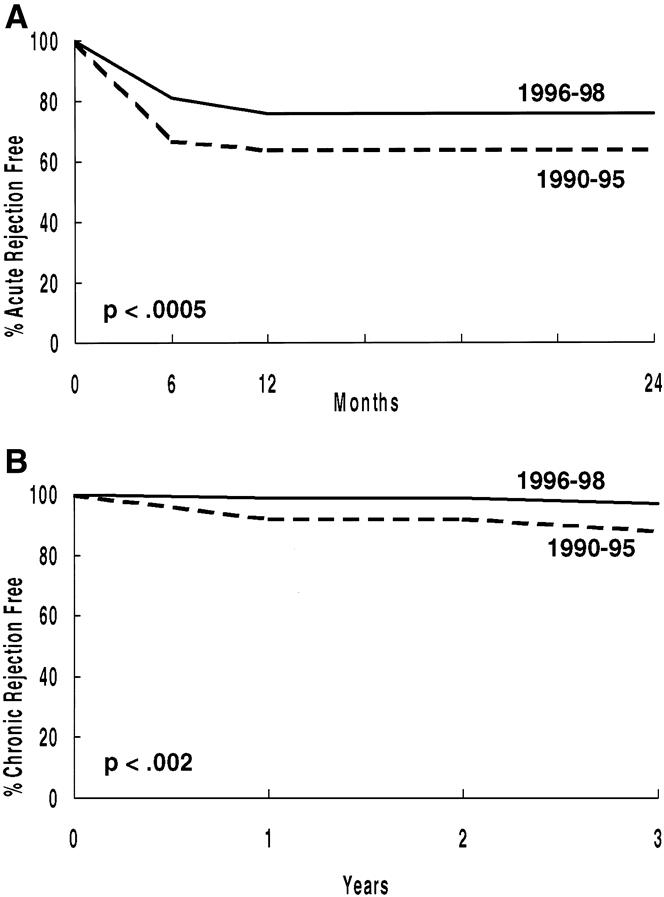
Results: For each decade since 1960, outcome has improved after living donor transplants. Compared with patients transplanted in the 1960s, those transplanted in the 1990s have better 8-year actuarial patient and graft survival rates. Death with function and chronic rejection have continued to be a major cause of graft loss, whereas acute rejection has become a rare cause of graft loss. Cardiovascular deaths have become a more predominant cause of patient death; infection has decreased. Donor source (e.g., ideally HLA-identical sibling) continues to be important. For living donor transplants, rejection and graft survival rates are related to donor source. The authors show that patients who had preemptive transplants or less than 1 year of dialysis have better 5-year graft survival and more frequently return to full-time employment. Readmission and complications remain problems; of patients transplanted in the 1990s, only 36% never required readmission. Similarly, steroid-related complications remain common. The authors' multivariate analysis shows that the major risk factor for worse 1-year graft survival was delayed graft function. For recipients with 1-year graft survival, risk factors for worse long-term outcome were pretransplant smoking, pretransplant peripheral vascular disease, pretransplant dialysis for more than 1 year, one or more acute rejection episodes, and donor age older than 55.
Conclusions: These data show that the outcome of living donor transplants has continued to improve. However, for living donors, donor source affects outcome. The authors also identify other major risk factors affecting both short- and long-term outcome.
Figures
References
-
- Murray JE, Merrill JP, Harrison JH. Renal homotransplantation in identical twins. Surg Forum 1955; 6: 432–436. - PubMed
-
- Merrill JP, Murray JE, Harrison JH, et al. Successful homotransplantation of the human kidney between identical twins. JAMA 1956; 160: 277–282. - PubMed
-
- Kries H. Why living donors should not be used whenever possible. Transplant Proc 1985; 17: 1510–1514.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
