

Is it possible to exclude a diagnosis of myocardial damage within six hours of admission to an emergency department? Diagnostic cohort study
- PMID: 11509427
- PMCID: PMC37396
- DOI: 10.1136/bmj.323.7309.372
Is it possible to exclude a diagnosis of myocardial damage within six hours of admission to an emergency department? Diagnostic cohort study
Abstract
Objective: To assess the clinical efficacy and accuracy of an emergency department based six hour rule-out protocol for myocardial damage.
Design: Diagnostic cohort study.
Setting: Emergency department of an inner city university hospital.
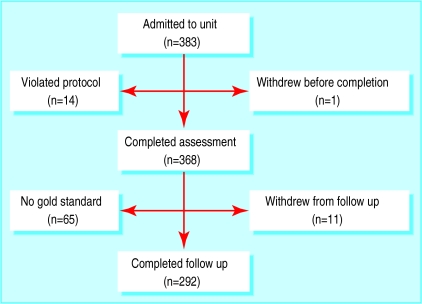
Participants: 383 consecutive patients aged over 25 years with chest pain of less than 12 hours' duration who were at low to moderate risk of acute myocardial infarction.
Intervention: Serial measurements of creatine kinase MB mass and continuous ST segment monitoring for six hours with 12 leads.
Main outcome measure: Performance of the diagnostic test against a gold standard consisting of either a 48 hour measurement of troponin T concentration or screening for myocardial infarction according to the World Health Organization's criteria.
Results: Outcome of the gold standard test was available for 292 patients. On the diagnostic test for the protocol, 53 patients had positive results and 239 patients had negative results. There were 18 false positive results and one false negative result. Sensitivity was 97.2% (95% confidence interval 95.0% to 99.0%), specificity 93.0% (90.0% to 96.0%), the negative predictive value 99.6%, and the positive predictive value 66.0%. The positive likelihood ratio was 13.9 and the negative likelihood ratio 0.03.
Conclusions: The six hour rule-out protocol for myocardial infarction is accurate and efficacious. It can be used in patients presenting to emergency departments with chest pain indicating a low to moderate risk of myocardial infarction.
Comment in
-
Diagnosing myocardial infarction. Additional tools may help to identify patients at low risk.BMJ. 2001 Dec 8;323(7325):1366. BMJ. 2001. PMID: 11776947 No abstract available.
References
-
- Emerson PA, Russell NJ, Wyatt J, Crichton N, Pantin CFA, Morgan AD, et al. An audit of doctors management of patients with chest pain in the accident and emergency department. Q J Med. 1989;70:213–220. - PubMed
-
- Lee TH, Rouan GW, Weisberg M, Brand DA, Cook EF, Acampora D, et al. Sensitivity of routine clinical criteria for diagnosing myocardial infarction within 24 hours of hospitalisation. Ann Intern Med. 1987;106:181–186. - PubMed
-
- Mair J, Artner-Dworzak E, Lechleitner P, Smidt J, Wagner I, Dienstl F, et al. Cardiac troponin T in diagnosis of acute myocardial infarction. Clin Chem. 1991;37:845–852. - PubMed
-
- ISIS-2 (Second international study of infarct survival) collaborative group. ISIS-2: a randomised comparison of streptokinase vs tissue plasminogen activator vs anistreplase and of aspirin plus heparin vs aspirin alone in 41299 cases of suspected acute myocardial infarction. Lancet. 1992;339:753–770. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous