

Cyclooxygenase 2-implications on maintenance of gastric mucosal integrity and ulcer healing: controversial issues and perspectives
- PMID: 11511570
- PMCID: PMC1728453
- DOI: 10.1136/gut.49.3.443
Cyclooxygenase 2-implications on maintenance of gastric mucosal integrity and ulcer healing: controversial issues and perspectives
Abstract
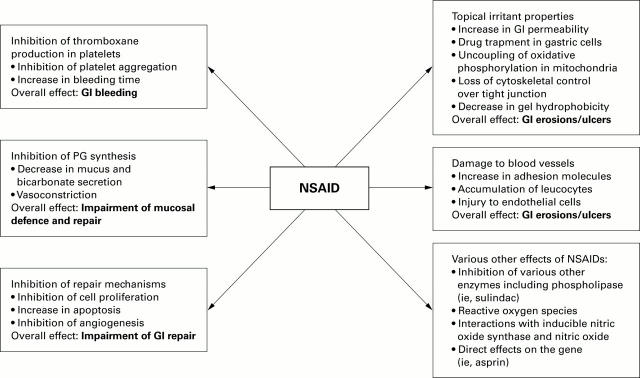
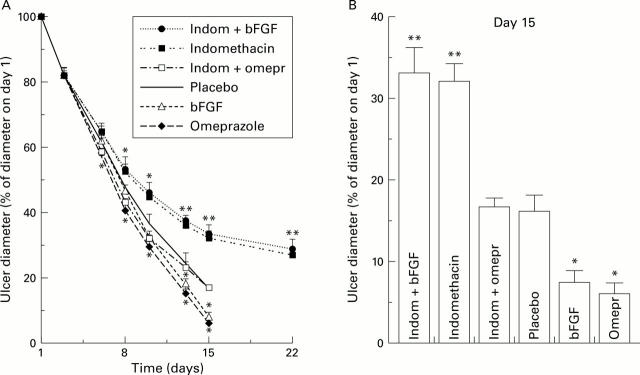
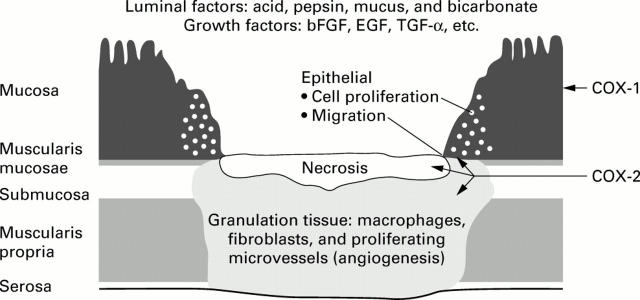
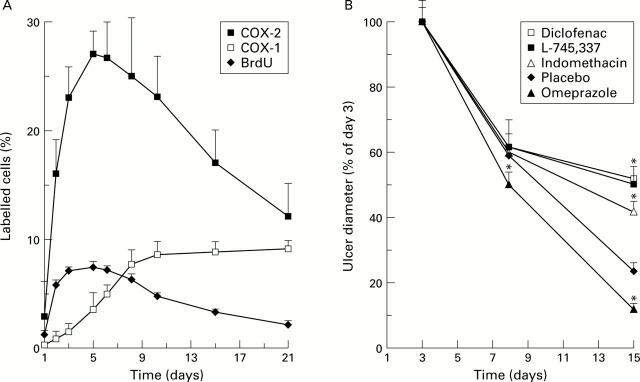
Cyclooxygenase (COX), the key enzyme for synthesis of prostaglandins, exists in two isoforms (COX-1 and COX-2). COX-1 is constitutively expressed in the gastrointestinal tract in large quantities and has been suggested to maintain mucosal integrity through continuous generation of prostaglandins. COX-2 is induced predominantly during inflammation. On this premise selective COX-2 inhibitors not affecting COX-1 in the gastrointestinal tract mucosa have been developed as gastrointestinal sparing anti-inflammatory drugs. They appear to be well tolerated by experimental animals and humans following acute and chronic (three or more months) administration. However, there is increasing evidence that COX-2 has a greater physiological role than merely mediating pain and inflammation. Thus gastric and intestinal lesions do not develop when COX-1 is inhibited but only when the activity of both COX-1 and COX-2 is suppressed. Selective COX-2 inhibitors delay the healing of experimental gastric ulcers to the same extent as non-COX-2 specific non-steroidal anti-inflammatory drugs (NSAIDs). Moreover, when given chronically to experimental animals, they can activate experimental colitis and cause intestinal perforation. The direct involvement of COX-2 in ulcer healing has been supported by observations that expression of COX-2 mRNA and protein is upregulated at the ulcer margin in a temporal and spatial relation to enhanced epithelial cell proliferation and increased expression of growth factors. Moreover, there is increasing evidence that upregulation of COX-2 mRNA and protein occurs during exposure of the gastric mucosa to noxious agents or to ischaemia-reperfusion. These observations support the concept that COX-2 represents (in addition to COX-1) a further line of defence for the gastrointestinal mucosa necessary for maintenance of mucosal integrity and ulcer healing.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials