

Defining the optimal surgeon experience for breast cancer sentinel lymph node biopsy: a model for implementation of new surgical techniques
- PMID: 11524582
- PMCID: PMC1422020
- DOI: 10.1097/00000658-200109000-00003
Defining the optimal surgeon experience for breast cancer sentinel lymph node biopsy: a model for implementation of new surgical techniques
Abstract
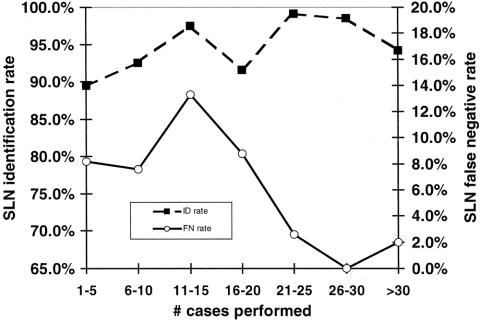
Objective: To determine the optimal experience required to minimize the false-negative rate of sentinel lymph node (SLN) biopsy for breast cancer.
Summary background data: Before abandoning routine axillary dissection in favor of SLN biopsy for breast cancer, each surgeon and institution must document acceptable SLN identification and false-negative rates. Although some studies have examined the impact of individual surgeon experience on the SLN identification rate, minimal data exist to determine the optimal experience required to minimize the more crucial false-negative rate.
Methods: Analysis was performed of a large prospective multiinstitutional study involving 226 surgeons. SLN biopsy was performed using blue dye, radioactive colloid, or both. SLN biopsy was performed with completion axillary LN dissection in all patients. The impact of surgeon experience on the SLN identification and false-negative rates was examined. Logistic regression analysis was performed to evaluate independent factors in addition to surgeon experience associated with these outcomes.
Results: A total of 2,148 patients were enrolled in the study. Improvement in the SLN identification and false-negative rates was found after 20 cases had been performed. Multivariate analysis revealed that patient age, nonpalpable tumors, and injection of blue dye alone for SLN biopsy were independently associated with decreased SLN identification rates, whereas upper outer quadrant tumor location was the only factor associated with an increased false-negative rate.
Conclusions: Surgeons should perform at least 20 SLN cases with acceptable results before abandoning routine axillary dissection. This study provides a model for surgeon training and experience that may be applicable to the implementation of other new surgical technologies.
Figures

References
-
- Giuliano AE. See one, do twenty-five, teach one: the implementation of sentinel node dissection in breast cancer. Ann Surg Oncol 1999; 6: 520–521. - PubMed
-
- Morton DL. Intraoperative lymphatic mapping and sentinel lymphadenectomy: community standard care or clinical investigation? Cancer J Sci Am 1997; 3: 328–330. - PubMed
-
- Tafra L, McMasters KM, Whitworth P, Edwards MJ. Credentialing issues with sentinel lymph node staging for breast cancer. Am J Surg 2000; 180: 268–273. - PubMed
-
- McMasters KM, Giuliano AE, Ross MI, et al. Sentinel lymph node biopsy for breast cancer: not yet the standard of care. N Engl J Med 1998; 339: 990–995. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
