

New paradigms and improved results for the surgical treatment of acute type A dissection
- PMID: 11524586
- PMCID: PMC1422024
- DOI: 10.1097/00000658-200109000-00007
New paradigms and improved results for the surgical treatment of acute type A dissection
Abstract
Objective: To examine the effect of an integrated surgical approach to the treatment of acute type A dissections.
Summary background data: Acute type A dissection requires surgery to prevent death from proximal aortic rupture or malperfusion. Most series of the past decade have reported a death rate in the range of 15% to 30%.
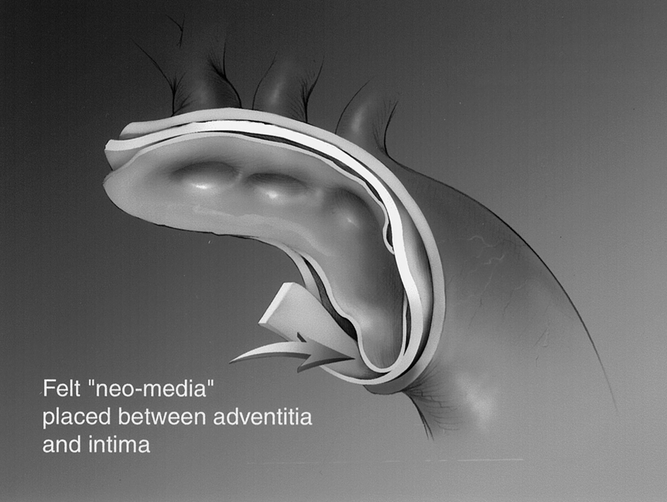
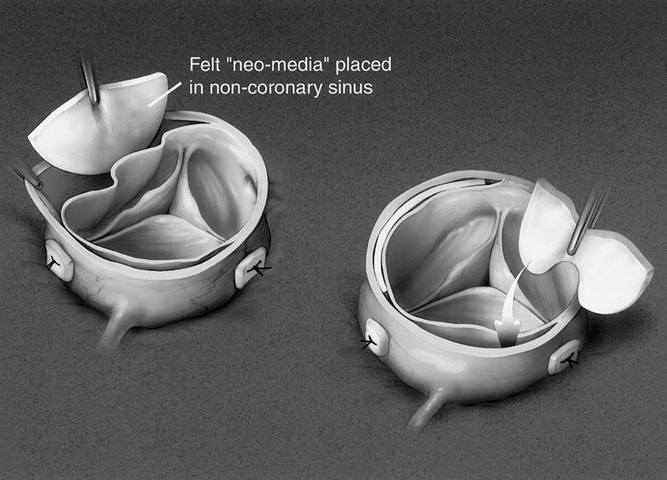
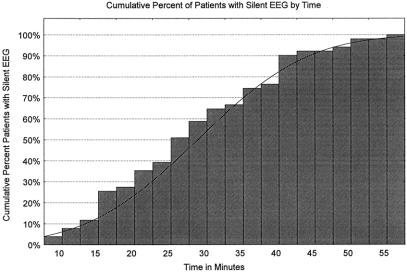
Methods: From January 1994 to March 2001, 104 consecutive patients underwent repair of acute type A dissection. All had an integrated operative management as follows: intraoperative transesophageal echocardiography; hypothermic circulatory arrest (HCA) with retrograde cerebral perfusion (RCP) to replace the aortic arch; HCA established after 5 minutes of electroencephalographic (EEG) silence in neuromonitored patients (66%) or after 45 minutes of cooling in patients who were not neuromonitored (34%); reinforcement of the residual arch tissue with a Teflon felt "neo-media"; cannulation of the arch graft to reestablish cardiopulmonary bypass at the completion of HCA (antegrade graft perfusion); and remodeling of the sinus of Valsalva segments with Teflon felt "neo-media" and aortic valve resuspension (78%) or replacement with a biologic or mechanical valved conduit (22%).
Results: Mean age was 59 +/- 15 (range 22-86) years, with 71% men and 13% redo sternotomy after a previous cardiac procedure. Mean cardiopulmonary bypass time was 196 +/- 50 minutes. Mean HCA with RCP time was 42 +/- 12 minutes (range 19-84). Mean cardiac ischemic time was 140 +/- 45 minutes. Eleven percent of patients presented with a preoperative neurologic deficit, and 5% developed a new cerebrovascular accident after dissection repair. The in-hospital death rate was 9%. Excluding the patients who presented neurologically unresponsive or with ongoing cardiopulmonary resuscitation (n = 5), the death rate was 4%. In six patients adverse cerebral outcomes were potentially avoided when immediate surgical fenestration was prompted by a sudden change in the EEG during cooling. Forty-five percent of neuromonitored patients required greater than 30 minutes to achieve EEG silence.
Conclusion: The authors have shown that the surgical integration of sinus segment repair or aortic root replacement, the use of EEG monitoring, partial or total arch replacement using RCP, routine antegrade graft perfusion, and the uniform use of transesophageal echocardiography substantially decrease the death and complication rates of acute type A dissection repair.
Figures
References
-
- Fuster V, Ip JF. Medical aspects of acute aortic dissection. Semin Thorac Cardiovasc Surg 1991; 3: 219–224. - PubMed
-
- Hagan PG, Nienaber CA, Isselbacher EM, et al. The international registry of acute aortic dissection (IRAD): new insights into an old disease. JAMA 2000; 283: 897–903. - PubMed
-
- Livesay JJ, Cooley DA, Duncan JM, et al. Open aortic anastomosis: improved results in the treatment of aneurysms of the aortic arch. Circulation 1982; 66 (suppl I): 122–127. - PubMed
-
- Lemole GM, Strong MD, Spagna PM, et al. Improved results for dissecting aneurysms: intraluminal sutureless prosthesis. J Thorac Cardiovasc Surg 1982; 83: 249–255. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
