

Clinical intestinal transplantation: a decade of experience at a single center
- PMID: 11524593
- PMCID: PMC1422031
- DOI: 10.1097/00000658-200109000-00014
Clinical intestinal transplantation: a decade of experience at a single center
Abstract
Objective: To assess the long-term efficacy of intestinal transplantation under tacrolimus-based immunosuppression and the therapeutic benefit of newly developed adjunct immunosuppressants and management strategies.
Summary background data: With the advent of tacrolimus in 1990, transplantation of the intestine began to emerge as therapy for intestinal failure. However, a high risk of rejection, with the consequent need for acute and chronic high-dose immunosuppression, has inhibited its widespread application.
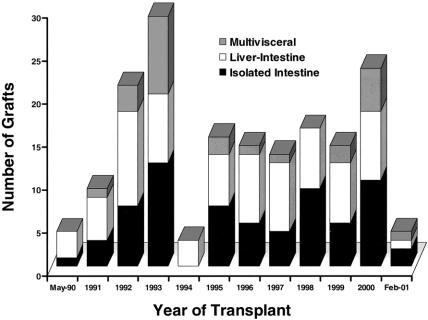
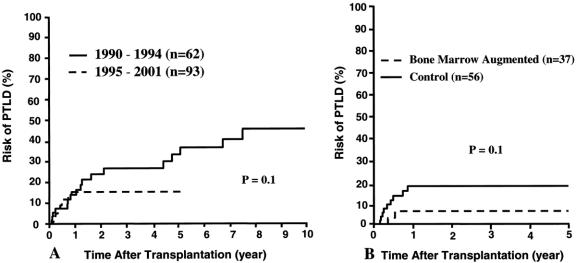
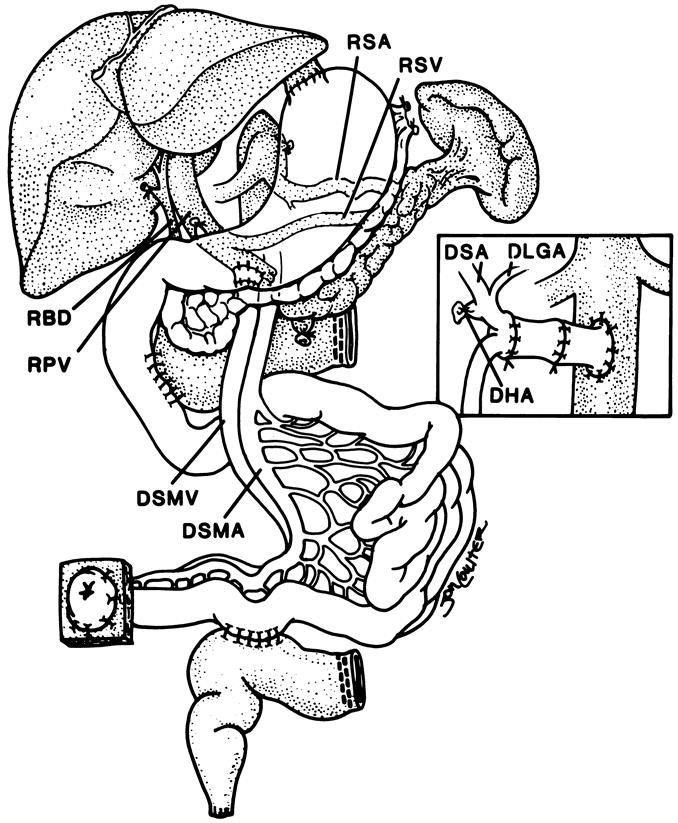
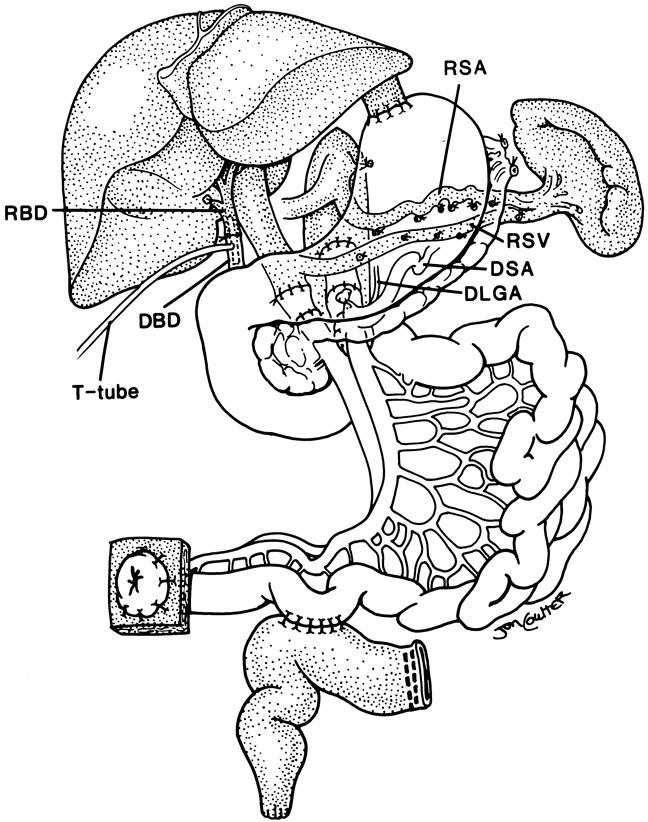
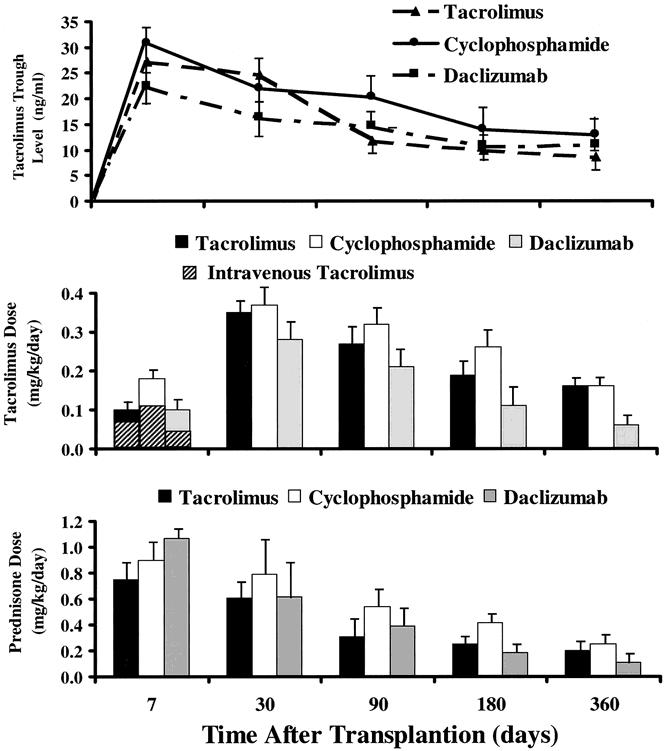
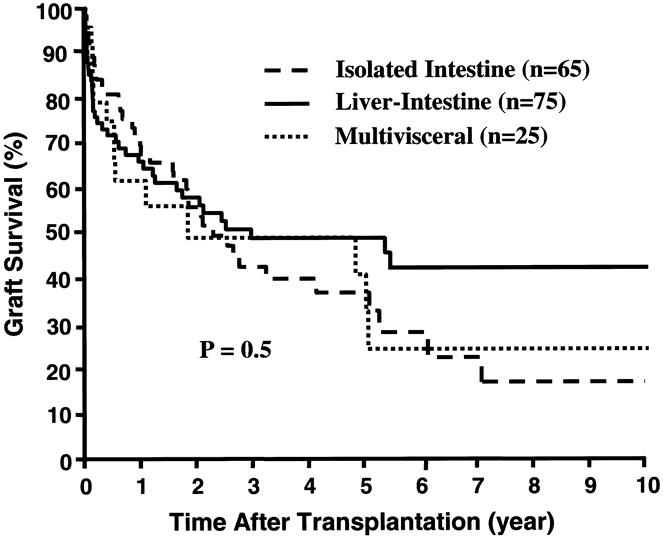
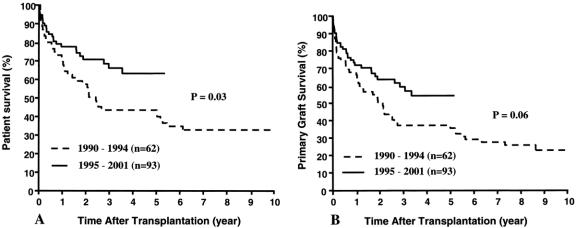
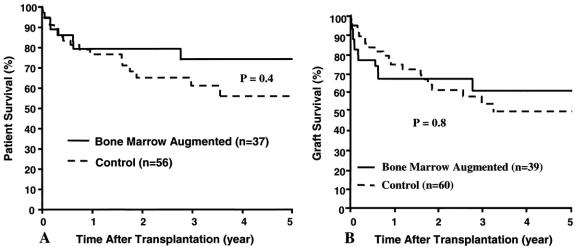
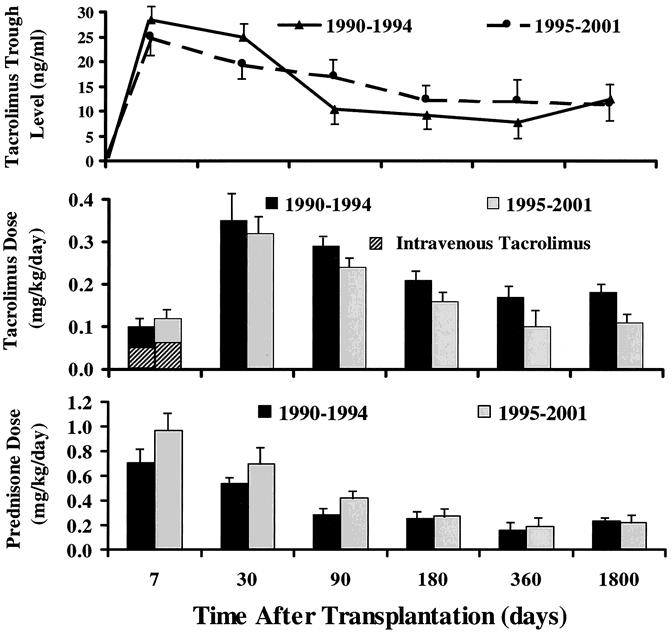
Methods: During an 11-year period, divided into two segments by a 1-year moratorium in 1994, 155 patients received 165 intestinal allografts under immunosuppression based on tacrolimus and prednisone: 65 intestine alone, 75 liver and intestine, and 25 multivisceral. For the transplantations since the moratorium (n = 99), an adjunct immunosuppressant (cyclophosphamide or daclizumab) was used for 74 transplantations, adjunct donor bone marrow was given in 39, and the intestine of 11 allografts was irradiated with a single dose of 750 cGy.
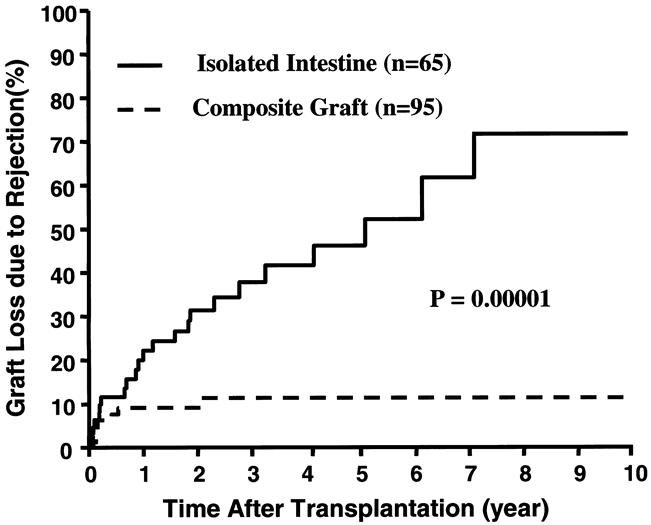
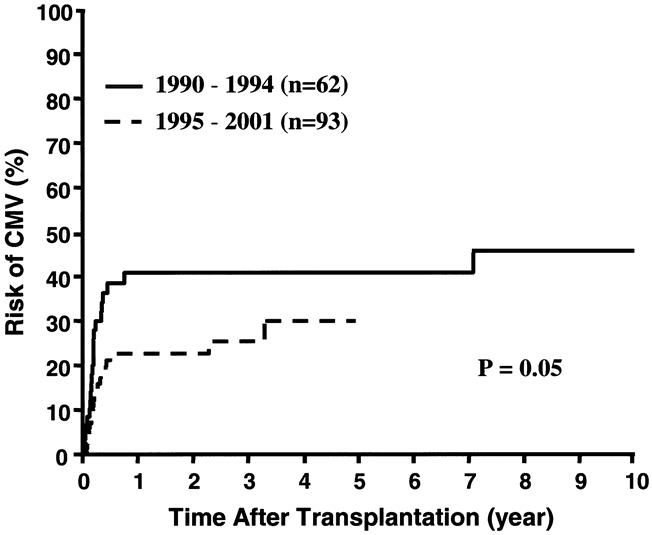
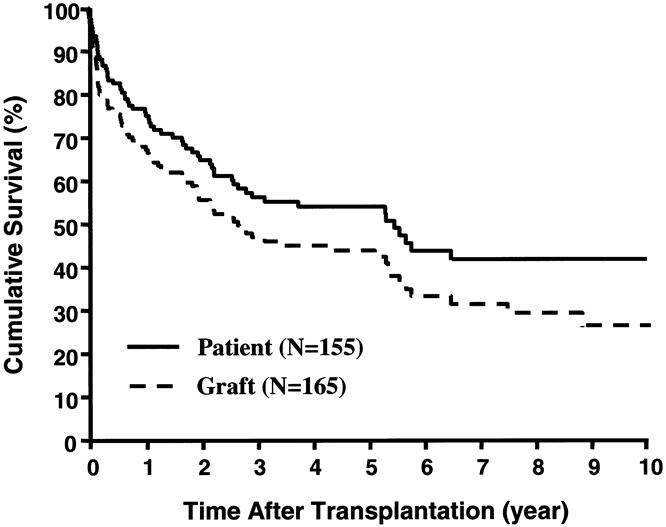
Results: The actuarial survival rate for the total population was 75% at 1 year, 54% at 5 years, and 42% at 10 years. Recipients of liver plus intestine had the best long-term prognosis and the lowest risk of graft loss from rejection (P =.001). Since 1994, survival rates have improved. Techniques for early detection of Epstein-Barr and cytomegaloviral infections, bone marrow augmentation, the adjunct use of the interleukin-2 antagonist daclizumab, and most recently allograft irradiation may have contributed to the better results.
Conclusion: The survival rates after intestinal transplantation have cumulatively improved during the past decade. With the management strategies currently under evaluation, intestinal transplant procedures have the potential to become the standard of care for patients with end-stage intestinal failure.
Figures
References
-
- Deltz E, Schroeder P, Gebhardt H, et al. Successful clinical small bowel transplantation: Report of a case. Clin Transplant 1989; 3: 89–91.
-
- Grant D, Wall W, Mimeault R, et al. Successful small-bowel/liver transplantation. Lancet 1990; 335: 181–184. - PubMed
-
- Margreiter R, Konigsrainer A, Schmid T, et al. Successful multivisceral transplantation. Transplant Proc 1992; 24: 1226–1227. - PubMed
-
- Goulet O, Revillon Y, Brousse N, et al. Successful small bowel transplantation in an infant. Transplantation 1992; 53: 940–943. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
