

Reliable detection of respiratory syncytial virus infection in children for adequate hospital infection control management
- PMID: 11526141
- PMCID: PMC88309
- DOI: 10.1128/JCM.39.9.3135-3139.2001
Reliable detection of respiratory syncytial virus infection in children for adequate hospital infection control management
Abstract
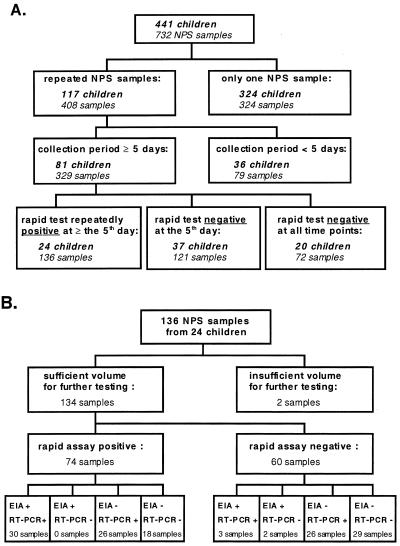
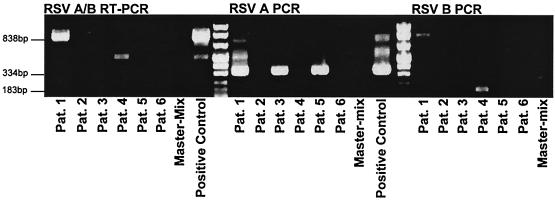
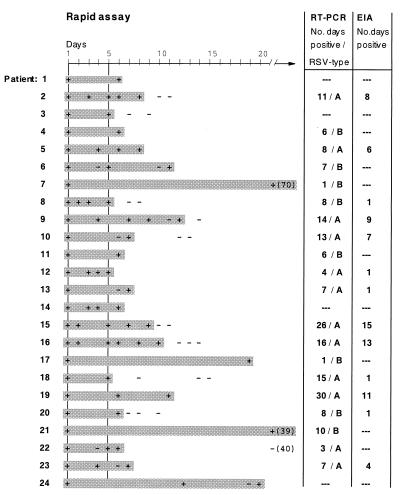
By using a rapid test for respiratory syncytial virus (RSV) detection (Abbott TestPack RSV), a number of patients were observed, showing repeatedly positive results over a period of up to 10 weeks. A prospective study was initiated to compare the rapid test with an antigen capture enzyme immunoassay (EIA) and a nested reverse transcriptase PCR (RT-PCR) protocol for detection of RSV serotypes A and B. Only respiratory samples from children exhibiting the prolonged presence of RSV (> or =5 days) as determined by the rapid test were considered. A total of 134 specimens from 24 children was investigated by antigen capture EIA and nested RT-PCR. Using RT-PCR as the reference method, we determined the RSV rapid test to have a specificity of 63% and a sensitivity of 66% and the antigen capture EIA to have a specificity of 96% and a sensitivity of 69% for acute-phase samples and the homologous virus serotype A. In 7 (29%) of 24 patients, the positive results of the RSV rapid test could not be confirmed by either nested RT-PCR or antigen capture EIA. In these seven patients a variety of other respiratory viruses were detected. For general screening the RSV rapid test was found to be a reasonable tool to get quick results. However, its lack of specificity in some patients requires confirmation by additional tests to rule out false-positive results and/or detection of other respiratory viruses.
Figures
References
-
- Fan J, Henrickson K J, Savatski L L. Rapid simultaneous diagnosis of infections with respiratory syncytial viruses A and B, influenza viruses A and B, and human parainfluenza virus type 1, 2, and 3 by multiplex quantitative reverse transcription-polymerase chain reaction-enzyme hybridization assay (Hexaplex) Clin Infect Dis. 1998;26:1397–1402. - PubMed
-
- Hall C B, Douglas R G, Geiman J M. Quantitative shedding patterns of respiratory syncytial virus in infants. J Infect Dis. 1975;132:151–156. - PubMed
-
- Krilov L R, Lipson S M, Barone S R, Kaplan M H, Ciamician Z, Harkness S H. Evaluation of a rapid diagnostic test for respiratory syncytial virus (RSV): potential for bedside diagnosis. Pediatrics. 1994;93:903–906. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
