

Adverse cardiac events after surgery: assessing risk in a veteran population
- PMID: 11556926
- PMCID: PMC1495256
- DOI: 10.1046/j.1525-1497.2001.016008507.x
Adverse cardiac events after surgery: assessing risk in a veteran population
Abstract
Objective: To establish rates of and risk factors for cardiac complications after noncardiac surgery in veterans.
Design: Prospective cohort study.
Setting: A large urban veterans affairs hospital.
Participants: One thousand patients with known or suspected cardiac problems undergoing 1,121 noncardiac procedures.
Measurements: Patients were assessed preoperatively for important clinical variables. Postoperative evaluation was done by an assessor blinded to preoperative status with a daily physical examination, electrocardiogram, and creatine kinase with MB fraction until postoperative day 6, day of discharge, death, or reoperation (whichever occurred earliest). Serial electrocardiograms, enzymes, and chest radiographs were obtained as indicated. Severe cardiac complications included cardiac death, cardiac arrest, myocardial infarction, ventricular tachycardia, and fibrillation and pulmonary edema. Serious cardiac complications included the above, heart failure, and unstable angina.
Main results: Severe and serious complications were seen in 24% and 32% of aortic, 8.3% and 10% of carotid, 11.8% and 14.7% of peripheral vascular, 9.0% and 13.1% of intraabdominal/intrathoracic, 2.9% and 3.3% of intermediate-risk (head and neck and major orthopedic procedures), and 0.27% and 1.1% of low-risk procedures respectively. The five associated patient-specific risk factors identified by logistic regression are: myocardial infarction < 6 months (odds ratio [OR], 4.5; 95% confidence interval [CI], 1.9 to 12.9), emergency surgery (OR, 2.6; 95% CI, 1.2 to 5.6), myocardial infarction > 6 months (OR, 2.2; 95% CI, 1.4 to 3.5), heart failure ever (OR, 1.9; 95% CI, 1.2 to 3.0), and rhythm other than sinus (OR, 1.7; 95% CI, 0.9 to 3.2). Inclusion of the planned operative procedure significantly improves the predictive ability of our risk model.
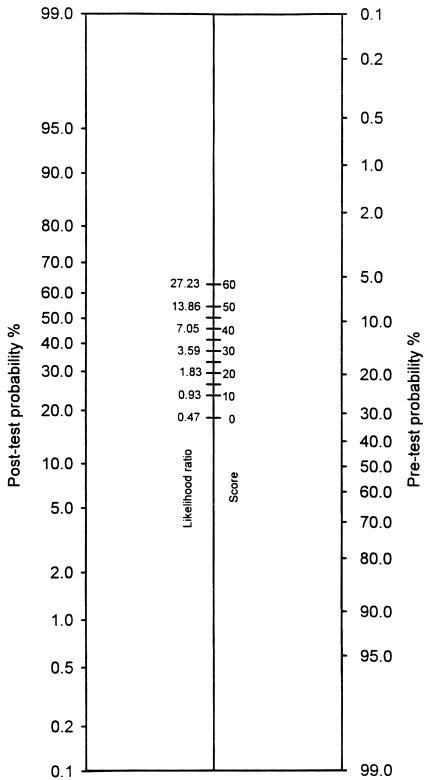
Conclusions: Five patient-specific risk factors are associated with high risk for cardiac complications in the perioperative period of noncardiac surgery in veterans. Inclusion of the operative procedure significantly improves the predictive ability of the risk model. Overall cardiac complication rates (pretest probabilities) are established for these patients. A simple nomogram is presented for calculation of post-test probabilities by incorporating the operative procedure.
Figures
References
-
- Goldman L, Caldera DL, Nussbaum SR, et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med. 1977;297:845–50. - PubMed
-
- Jeffrey CC, Kunsman J, Cullen DJ, Brewster DC. A prospective evaluation of cardiac risk index. Anesthesiology. 1983;58:462–4. - PubMed
-
- Detsky AS, Abrams HB, McLaughlin JR, et al. Predicting cardiac complication in patients undergoing non-cardiac surgery. J Gen Intern Med. 1986;1:211–9. - PubMed
-
- Mangano DT, Browner WS, Hollenberg M, London MJ, Tubau JF, Tateo MS. Association of perioperative myocardial ischemia with cardiac morbidity and mortality in men undergoing noncardiac surgery. N Engl J Med. 1990;323:1781–8. - PubMed
-
- Ashton CM, Peterson NJ, Wray NP, et al. The incidence of perioperative myocardial infarction in men undergoing noncardiac surgery. Ann Intern Med. 1993;118:504–10. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous