

Conservative management of persistent postnatal urinary and faecal incontinence: randomised controlled trial
- PMID: 11557703
- PMCID: PMC55571
- DOI: 10.1136/bmj.323.7313.593
Conservative management of persistent postnatal urinary and faecal incontinence: randomised controlled trial
Abstract
Objectives: To assess the effect of nurse assessment with reinforcement of pelvic floor muscle training exercises and bladder training compared with standard management among women with persistent incontinence three months postnatally.
Design: Randomised controlled trial with nine months' follow up.
Setting: Community intervention in three centres (Dunedin, New Zealand; Birmingham; Aberdeen).
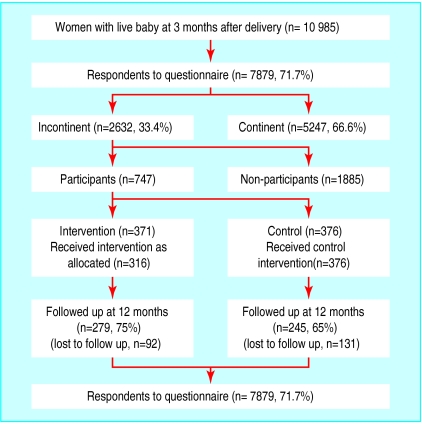
Participants: 747 women with urinary incontinence three months postnatally, allocated at random to intervention (371) or control (376) groups.
Intervention: Assessment by nurses of urinary incontinence with conservative advice on pelvic floor exercises at five, seven, and nine months after delivery supplemented with bladder training if appropriate at seven and nine months.
Main outcome measures: Primary: persistence and severity of urinary incontinence 12 months after delivery. Secondary: performance of pelvic floor exercises, change in coexisting faecal incontinence, wellbeing, anxiety, and depression.
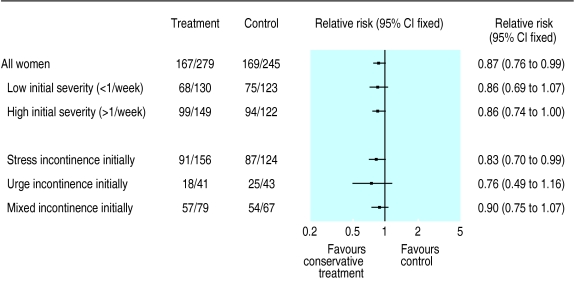
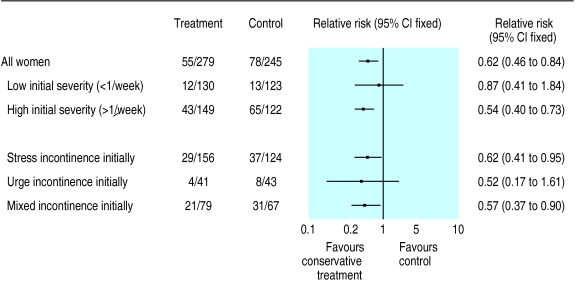
Results: Women in the intervention group had significantly less urinary incontinence: 167/279 (59.9%) v 169/245 (69.0%), difference 9.1% (95% confidence interval 1.0% to 17.3%, P=0.037) for any incontinence and 55/279 (19.7%) v 78/245 (31.8%), difference 12.1% (4.7% to 19.6%, P=0.002) for severe incontinence. Faecal incontinence was also less common: 12/273 (4.4%) v 25/237 (10.5%), difference 6.1% (1.6% to 10.8%, P=0.012). At 12 months women in the intervention group were more likely to be performing pelvic floor exercises (218/278 (79%) v 118/244 (48%), P<0.001).
Conclusions: A third of women may have some urinary incontinence three months after childbirth. Conservative management provided by nurses seems to reduce the likelihood of urinary and coexisting faecal incontinence persisting 12 months postpartum. Further trials for faecal incontinence are needed.
Figures
References
-
- MacArthur C, Lewis M, Knox EG. Health after childbirth. London: HMSO; 1991. - PubMed
-
- Wilson PD, Herbison RM, Herbison GP. Obstetric practice and the prevalence of urinary incontinence three months after delivery. Br J Obstet Gynaecol. 1996;103:154–161. - PubMed
-
- MacArthur C, Lewis M, Bick D. Stress incontinence after childbirth. Br J Midwifery. 1993;1:207–215.
-
- MacArthur C, Bick DE, Keighley MRB. Faecal incontinence after childbirth. Br J Obstet Gynaecol. 1997;104:46–50. - PubMed
-
- Sultan AH, Kamm MA, Hudson CN, Thomas JM, Bartram CI. Anal-sphincter disruption during vaginal delivery. N Engl J Med. 1993;329:1905–1911. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical