

Quality improvement report: Linking guideline to regular feedback to increase appropriate requests for clinical tests: blood gas analysis in intensive care
- PMID: 11557715
- PMCID: PMC1121188
- DOI: 10.1136/bmj.323.7313.620
Quality improvement report: Linking guideline to regular feedback to increase appropriate requests for clinical tests: blood gas analysis in intensive care
Erratum in
- BMJ 2001 Oct 27;323(7319):993
Abstract
Problem: Need to decrease the number of requests for arterial blood gas analysis and increase their appropriateness to reduce the amount of blood drawn from patients, the time wasted by nurses, and the related cost.
Design: Assessment of the impact of a multifaceted intervention aimed at changing requests for arterial blood gas analysis in a before and after study.
Background and setting: Twenty bed surgical intensive care unit of a tertiary university affiliated hospital, receiving 1500 patients per year.
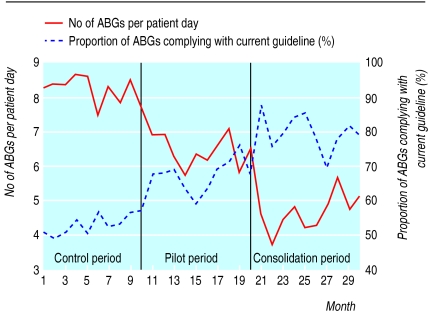
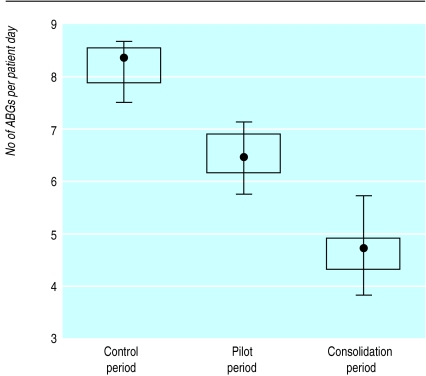
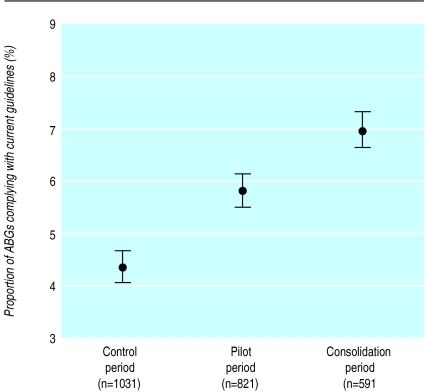
Key measures for improvement: Number of tests per patient day, proportion of tests complying with current guideline, and safety indicators (mortality, incident rate, length of stay). Comparison of three 10 month periods corresponding to baseline, pilot (first version of the guideline), and consolidated (second version of the guideline) periods from March 1997 to August 1999.
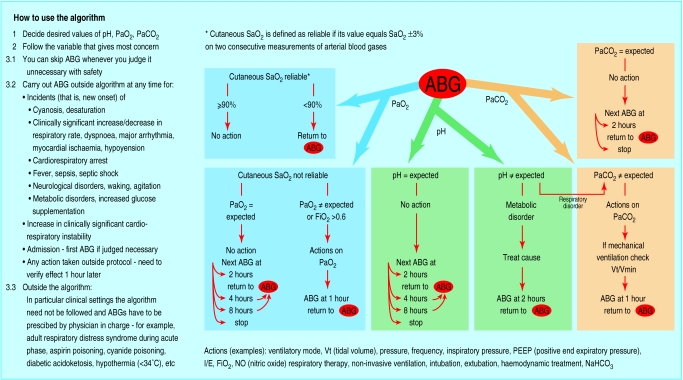
Strategies for change: Multifaceted intervention combining a new guideline developed by a multidisciplinary group, educational sessions, and monthly feedback about adherence to the guideline and use of blood gas analysis.
Effects of change: Substantial decrease in the number of tests per patient day (from 8.2 to 4.8; P<0.0001), associated with increased adherence to the guideline (from 53% to 80%, P<0.0001). No significant variation of safety indicators.
Lessons learnt: A multifaceted intervention can substantially decrease the number of requests for arterial blood gas analysis and increase their appropriateness without affecting patient safety.
Figures
References
-
- Klepzig H, Winten G, Thierolf C, Kiesling G, Usadel KH, Zeiher AM. Treatment costs in a medical intensive care unit: a comparison of 1992 and 1997 (in German) Dtsch Med Wochenschr. 1998;123:719–725. - PubMed
-
- Noseworthy TW, Konopad E, Shustack A, Johnston R, Grace M. Cost accounting of adult intensive care: methods and human and capital inputs. Crit Care Med. 1996;24:1168–1172. - PubMed
-
- Singer M, Myers S, Hall G, Cohen SL, Armstrong RF. The cost of intensive care: a comparison on one unit between 1988 and 1991. Intensive Care Med. 1994;20:542–549. - PubMed
-
- Eyster E, Bernene J. Nosocomial anemia. JAMA. 1973;223:73–74. - PubMed
-
- Henry ML, Garner WL, Fabri PJ. Iatrogenic anemia. Am J Surg. 1986;151:362–363. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials