

CT and MR imaging features of pyogenic ventriculitis
- PMID: 11559498
- PMCID: PMC7974570
CT and MR imaging features of pyogenic ventriculitis
Abstract
Background and purpose: Pyogenic ventriculitis is an uncommon manifestation of severe intracranial infection that might be clinically obscure. We hypothesized that determining characteristic imaging features of pyogenic ventriculitis in patients with appropriate risk factors might improve recognition of this severe infection.
Methods: Review of the medical records from 1990 to 2000 revealed 17 cases (12 men, five women) that satisfied inclusion criteria of abscess (n = 3) and/or positive cultures or increased white cells and protein in ventricular (n = 12) or cisternal (n = 1) cerebrospinal fluid. In one case, the diagnosis of ventriculitis was based on the combination of bacterial growth in lumbar cerebrospinal fluid and follow-up imaging. Staphylococcus species and Enterobacter species were the most common organisms. Two neuroradiologists independently evaluated imaging studies for hydrocephalus, ventricular debris, periventricular attenuation or signal abnormality, ependymal enhancement, and signs of meningitis or abscess. Sixteen studies in 11 patients were performed after the intravenous administration of contrast material.
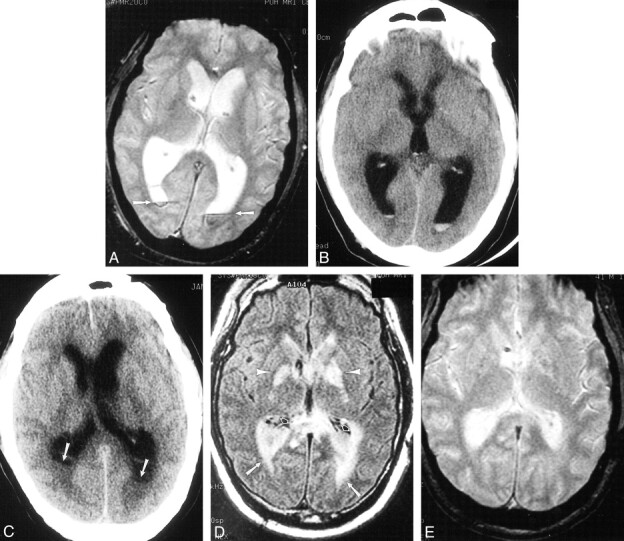
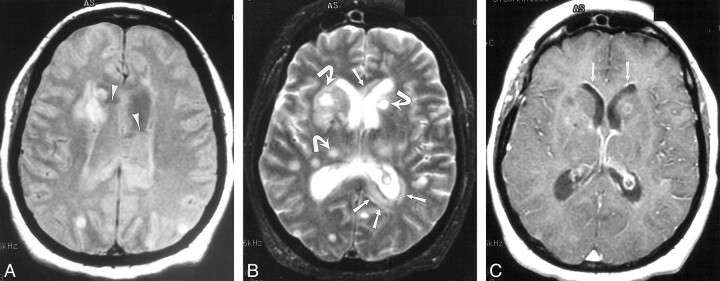
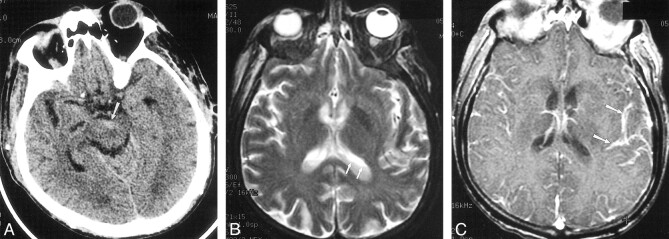
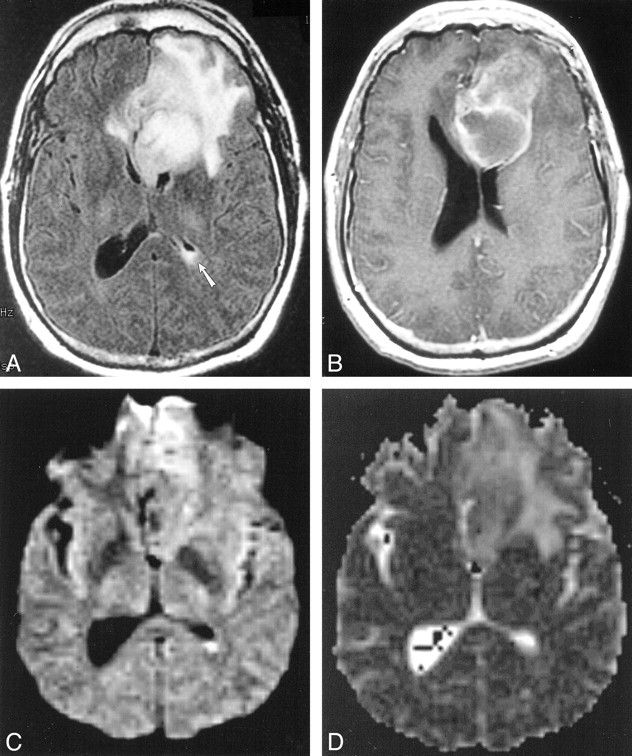
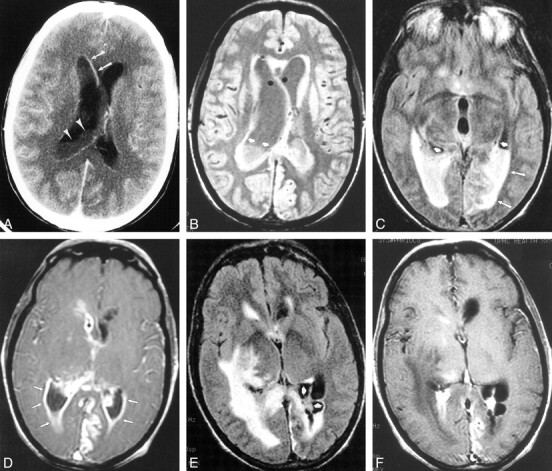
Results: Ventricular debris was detected in 16 (94%) of 17 cases and was irregular in 13 (81%) of 16 cases. Hydrocephalus was present in 13 (76%) of 17 cases. Periventricular hyperintense signal was present in most (seven [78%] of nine) cases with MR imaging and was most conspicuous on fluid-attenuated inversion recovery sequences. Ependymal enhancement was detected in seven (64%) of 11 cases in which contrast material was administered. Signs of meningitis (eg, pial or duraarachnoid signal abnormality or enhancement) were present in 13 (76%) of 17 cases. Three cases had imaging signs of abscess.
Conclusion: Ventricular debris was the most frequent sign of ventriculitis in this series. An irregular level was characteristic of debris in ventriculitis. Hydrocephalus and ependymal enhancement were less frequent signs. Detection of ventricular debris might facilitate diagnosis of pyogenic ventriculitis, a potentially fatal infection, and thus permit appropriate therapy.
Figures
References
-
- Bakshi R, Kinkel P, Mechtler L, et al. Cerebral ventricular empyema associated with severe adult pyogenic meningitis: computed tomography findings. Clin Neurol Neurosurg 1997;99:252-255 - PubMed
-
- Barloon TJ, Yuh WT, Knepper LE, et al. Cerebral ventriculitis: MR findings. J Comput Assist Tomogr 1990;14:272-275 - PubMed
-
- Bodino J, Lylyk P, Del Valle M, et al. Computed tomography in purulent meningitis. Am J Dis Child 1982;136:495-501 - PubMed
-
- Wormser G, Strashun A. Ventriculitis complicating gram negative meninigitis in an adult: diagnosis by radioisotope brain scanning and computerized tomography. Mt Sinai J Med 1980;47:575-578 - PubMed
-
- Vachon L, Mikity V. Computed tomography and ultrasound in purulent ventriculitis. J Ultrasound Med 1987;6:269-271 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical