

Review
Oculomotor nerve teratoma
AJNR Am J Neuroradiol.
2001 Sep.
Abstract
The case of a rare, mature teratoma of the oculomotor nerve manifesting as an interpeduncular cistern mass is presented. A basilar tip aneurysm initially was suspected on the basis of lesion location and MR imaging appearance. Subsequent CT and catheter angiography studies were atypical for aneurysm, leading to surgical biopsy. Pathologic analysis revealed a well-circumscribed mass composed of mature representatives of all three major cell lines characteristic of mature teratoma. The imaging findings are described, and a brief literature review is provided.
Figures
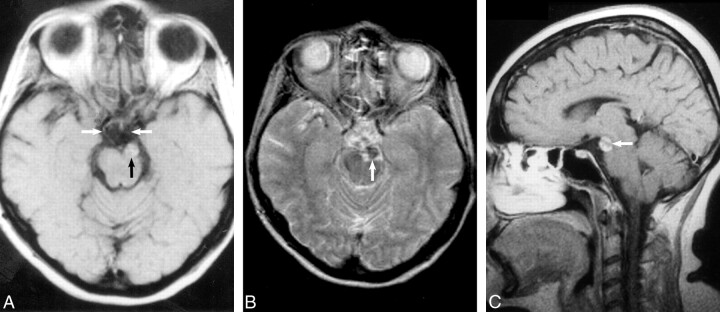
A, Axial T1-weighted unenhanced spin-echo image (800/25/3 [TR/TE/excitations]) demonstrates an extraaxial mass (black arrow) within the interpeduncular cistern that compresses the left cerebral peduncle and displaces the left oculomotor nerve medially (white arrows indicate the oculomotor nerves). The mass contains heterogeneous foci of high signal intensity. B, Conventional spin-echo axial T2-weighted image (2400/100/2) confirms a heterogeneous intermediate mass with low signal intensity (arrow) inseparable from the terminal basilar and left posterior cerebral arteries. C, Sagittal enhanced T1-weighted image (550/25/4) following intravenous administration of gadopentetate dimeglumine confirms heterogeneous enhancement (arrow) and normal suprasellar and pineal region cisterns.
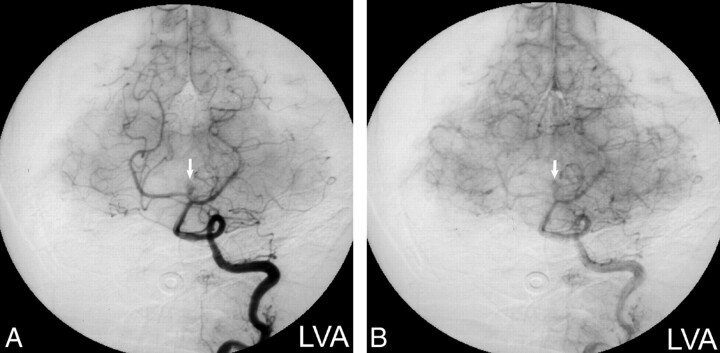
Digital subtraction angiograms. A, Left vertebral artery injection (arterial phase) shows vascular enhancement of the mass (arrow) in a pattern atypical for aneurysm. B, Left vertebral artery injection (capillary phase) confirms a persistent blush (arrow) that would be unusual for an aneurysm.
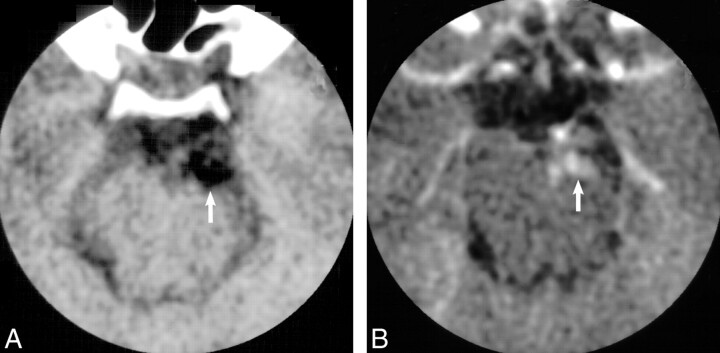
A, Axial nonenhanced CT image confirms that the mass (arrow) is hypoattenuating (−8 HU) compared with adjacent cerebrospinal fluid (6 HU) and noncalcified. B, Following intravenous administration of contrast material, the mass (arrow) reveals heterogeneous nodular enhancement (28–70 HU).
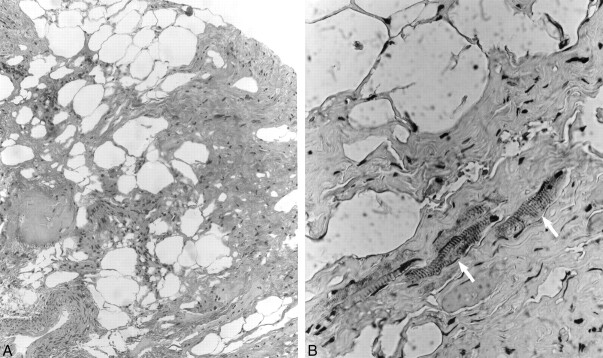
A, Low-power (original magnification ×100) H&E photomicrograph demonstrates dense collagen bundles admixed with fat cells, nerve filaments, and blood vessels. B, Higher power (original magnification ×400) immunoperoxidase (anti-desmin) preparation reveals scattered skeletal muscle fibers (arrows) interspersed within the dense collagenous tissue, features consistent with teratoma.
References
-
- Biousse V, Newman N. Third nerve palsies. Semin Neurol 2000;20:55-74 - PubMed
-
- Bianchi-Marzoli S, Brancato R. Third, fourth, and sixth cranial nerve palsies. Curr Opin Ophthalmol 1997;8:45-51 - PubMed
-
- Miller N. Solitary oculomotor nerve palsy in childhood. Am J Ophthalmol 1977;83:106-111 - PubMed
-
- Rucker C. The causes of paralysis of the third, fourth and sixth cranial nerves. Am J Ophthalmol 1966;61:1293-1298 - PubMed
-
- Okamoto S, Handa H, Yamashita J. Neurinoma of the oculomotor nerve. Surg Neurol 1985;4:275-278 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources