

Six year experience of transvenous left ventricular lead implantation for permanent biventricular pacing in patients with advanced heart failure: technical aspects
- PMID: 11559679
- PMCID: PMC1729936
- DOI: 10.1136/heart.86.4.405
Six year experience of transvenous left ventricular lead implantation for permanent biventricular pacing in patients with advanced heart failure: technical aspects
Abstract
Background: Biventricular pacing has been proposed as an adjuvant to optimal medical treatment in patients with drug refractory heart failure caused by chronic left ventricular systolic dysfunction and intraventricular conduction delay.
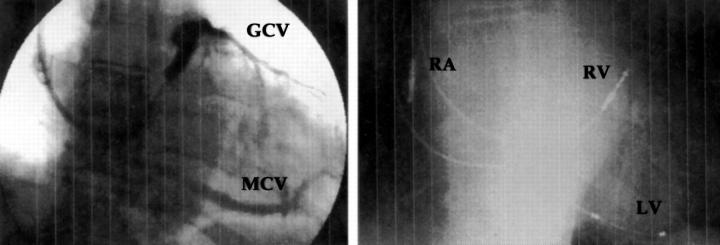
Objective: To assess the technical feasibility and long term results (over six years) of transverse left ventricular pacing with the lead inserted into a tributary vein of the coronary sinus.
Subjects: From August 1994 to February 2000, left ventricular lead implantation was attempted in 116 patients who were eligible for biventricular pacing (mean (SD) age 67 (9) years, New York Heart Association (NYHA) functional class III/IV, left ventricular ejection fraction 22 (6)%, QRS duration 185 (26) ms).
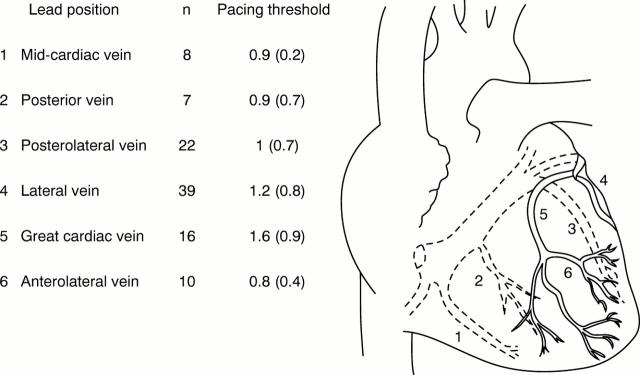
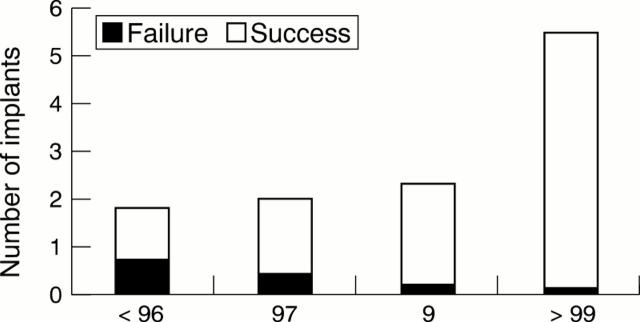
Results: The overall implantation success rate was 88% (n = 102). A learning curve was indicated by a progressive increase in success from 61% early on to 98% in the last year. The mean pacing threshold was 1.1 (0.7) V/0.5 ms at the time of implantation and increased slightly up to 1.9 (0.9) V/0.5 ms at the end of the follow up period (15 (13) months). The rate of acute and delayed left ventricular lead dislodgement decreased from 30% in the early years to 11% after 1999. During follow up, 19 patients required reoperation for delayed lead dislodgement or increase in left ventricular pacing threshold (n = 15), phrenic nerve stimulation (n = 3), or infection (n = 3).
Conclusions: Transverse left ventricular pacing through the coronary sinus is feasible and safe. The rate of implantation failure and of lead related problems has decreased greatly with increasing experience and with improvements in the equipment.
Figures
Similar articles
-
Biventricular pacing improves quality of life and exercise tolerance in patients with heart failure and intraventricular conduction delay.Can J Cardiol. 2002 Apr;18(4):380-7. Can J Cardiol. 2002. PMID: 11992131
-
Surgical epicardial left ventricular lead versus coronary sinus lead placement in biventricular pacing.Eur J Cardiothorac Surg. 2005 Feb;27(2):235-42. doi: 10.1016/j.ejcts.2004.09.029. Eur J Cardiothorac Surg. 2005. PMID: 15691676
-
[Biventricular pacing as a treatment for advanced heart failure. Preliminary experience in a series of 22 consecutive patients].Rev Esp Cardiol. 2003 Mar;56(3):245-52. doi: 10.1016/s0300-8932(03)76860-2. Rev Esp Cardiol. 2003. PMID: 12622954 Spanish.
-
[Biventricular cardiac pacing].Vnitr Lek. 2003 Sep;49(9):734-9. Vnitr Lek. 2003. PMID: 14584425 Review. Czech.
-
[Resynchronization therapy of heart failure].Magy Seb. 2007 Jan;60(1):481-7. doi: 10.1556/MaSeb.60.2007.1.3. Magy Seb. 2007. PMID: 17474300 Review. Hungarian.
Cited by
-
Central sleep apnea and atrial fibrillation: A review on pathophysiological mechanisms and therapeutic implications.Int J Cardiol Heart Vasc. 2020 May 22;30:100527. doi: 10.1016/j.ijcha.2020.100527. eCollection 2020 Oct. Int J Cardiol Heart Vasc. 2020. PMID: 33102683 Free PMC article. Review.
-
Noninvasive assessment of the biventricular pacing system.Ann Noninvasive Electrocardiol. 2004 Jan;9(1):58-70. doi: 10.1111/j.1542-474x.2004.91525.x. Ann Noninvasive Electrocardiol. 2004. PMID: 14731217 Free PMC article. Review. No abstract available.
-
Cardiac Resynchronization Therapy Using Quadripolar Versus Non-Quadripolar Left Ventricular Leads Programmed to Biventricular Pacing With Single-Site Left Ventricular Pacing: Impact on Survival and Heart Failure Hospitalization.J Am Heart Assoc. 2017 Oct 17;6(10):e007026. doi: 10.1161/JAHA.117.007026. J Am Heart Assoc. 2017. PMID: 29042422 Free PMC article.
-
Phrenic Nerve Stimulation for the Treatment of Central Sleep Apnea: A Pooled Cohort Analysis.J Clin Sleep Med. 2019 Dec 15;15(12):1747-1755. doi: 10.5664/jcsm.8076. Epub 2019 Nov 5. J Clin Sleep Med. 2019. PMID: 31855160 Free PMC article.
-
[From guiding catheter to coronary sinus lead].Herzschrittmacherther Elektrophysiol. 2006;17 Suppl 1:I7-13. doi: 10.1007/s00399-006-1102-z. Herzschrittmacherther Elektrophysiol. 2006. PMID: 16598625 German.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical