

GM-CSF and IL-2 induce specific cellular immunity and provide protection against Epstein-Barr virus lymphoproliferative disorder
- PMID: 11560958
- PMCID: PMC200931
- DOI: 10.1172/JCI12932
GM-CSF and IL-2 induce specific cellular immunity and provide protection against Epstein-Barr virus lymphoproliferative disorder
Abstract
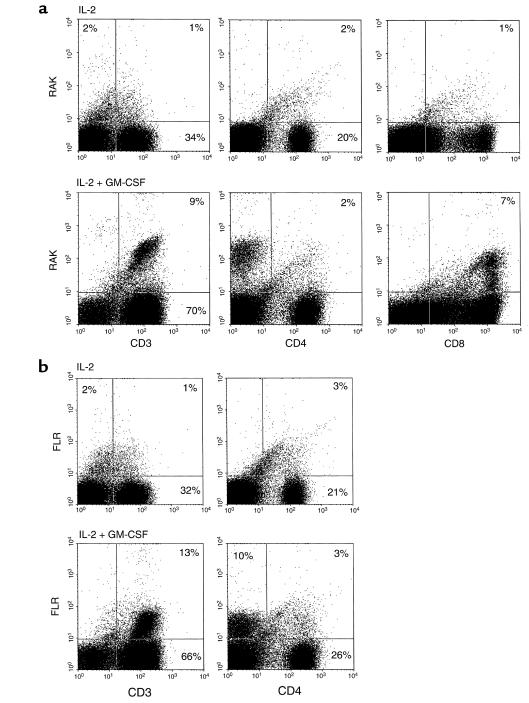
Epstein-Barr virus-associated lymphoproliferative disease (EBV-LPD) is a potentially life-threatening complication in immune-deficient patients. We have used the severe combined immune deficient (SCID) mouse engrafted with human leukocytes (hu-PBL-SCID) to evaluate the use of human cytokines in the prevention of EBV-LPD in vivo. Daily low-dose IL-2 therapy can prevent EBV-LPD in the hu-PBL-SCID mouse, but protection is lost if murine natural killer (NK) cells are depleted. Here we demonstrate that combined therapy with human GM-CSF and low-dose IL-2 is capable of preventing EBV-LPD in the hu-PBL-SCID mouse in the absence of murine NK cells. Lymphocyte depletion experiments showed that human NK cells, CD8(+) T cells, and monocytes were each required for the protective effects of GM-CSF and IL-2 combination therapy. This treatment resulted in a marked expansion of human CD3(+)CD8(+) lymphocytes in vivo. Using HLA tetramers complexed with EBV immunodominant peptides, a subset of these lymphocytes was found to be EBV-specific. These data establish that combined GM-CSF and low-dose IL-2 therapy can prevent the immune deficiencies that lead to fatal EBV-LPD in the hu-PBL-SCID mouse depleted of murine NK cells, and they point to a critical role for several human cellular subsets in mediating this protective effect.
Figures


Comment in
-
Are natural killer cells the key to treating Epstein-Barr virus-associated lymphoproliferative disorders?J Clin Invest. 2001 Sep;108(6):801-2. doi: 10.1172/JCI14003. J Clin Invest. 2001. PMID: 11560947 Free PMC article. Review. No abstract available.
References
-
- Liebowitz D. Epstein-Barr virus and a cellular signaling pathway in lymphomas from immunosuppressed patients. N Engl J Med. 1998;338:1413–1421. - PubMed
-
- Lucas KG, Small TN, Heller G, Dupont B, O’Reilly RJ. The development of cellular immunity to Epstein-Barr virus after allogeneic bone marrow transplantation. Blood. 1996;87:2594–2603. - PubMed
-
- Porcu P, et al. Post-transplant lymphoproliferative disorders following renal allografting: prospective immunological and molecular monitoring identifies correlates of clinical response to reduction of immune suppression and antiviral therapy. Proc Am Assoc Cancer Res. 2001;42:S84 . (Abstr.)
-
- Khatri VP, et al. Endogenous CD8+ T cell expansion during Epstein-Barr virus-associated posttransplant lymphoproliferative disorder. J Immunol. 1999;163:500–506. - PubMed
-
- Swinnen LJ. Diagnosis and treatment of transplant-related lymphoma. Ann Oncol. 2000;11:S45–S48. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
