

Delirium in older medical inpatients and subsequent cognitive and functional status: a prospective study
- PMID: 11563209
- PMCID: PMC81415
Delirium in older medical inpatients and subsequent cognitive and functional status: a prospective study
Abstract
Background: Delirium in older hospital inpatients appears to be associated with various adverse outcomes. The limitations of previous research on this association have included small sample sizes, short follow-up periods and lack of consideration of important confounders or modifiers, such as severity of illness, comorbidity and dementia. The objective of this study was to determine the prognostic significance of delirium, with or without dementia, for cognitive and functional status during the 12 months after hospital admission, independent of premorbid function, comorbidity, severity of illness and other potentially confounding variables.
Methods: Patients 65 years of age and older who were admitted from the emergency department to the medical services were screened for delirium during their first week in hospital. Two cohorts were enrolled: patients with prevalent or incident delirium and patients without delirium, but similar in age and cognitive impairment. The patients were followed up at 2, 6 and 12 months after hospital admission. Analyses were conducted for 4 patient groups: 56 with delirium, 53 with dementia, 164 with both conditions and 42 with neither. Baseline measures included delirium (Confusion Assessment Method), dementia (Informant Questionnaire on Cognitive Decline in the Elderly), physical function (Barthel Index [BI] and premorbid instrumental activities of daily living, IADL), the Mini-Mental State Examination (MMSE), comorbidity, and physiologic and clinical severity of illness. Outcome variables measured at follow-up were the MMSe, Barthel Index, IADL and admission to a long-term care facility.
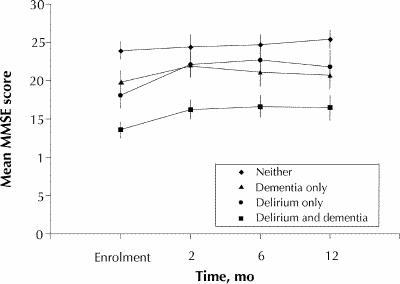
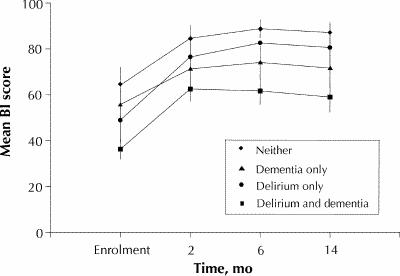
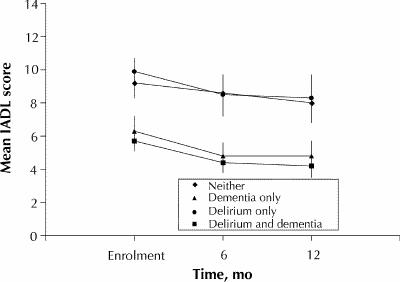
Results: After adjustment for covariates, the mean differences in MMSE scores at follow-up between patients with and without delirium were -4.99 (95% confidence interval [CI] -7.17 to -2.81) for patients with dementia and -3.36 (95% CI -6.15 to -0.58) for those without dementia. At 12 months, the adjusted mean differences in the BI were -16.45 (95% CI -27.42 to -5.50) and -13.89 (95% CI -28.39 to 0.61) for patients with and without dementia respectively. Patients with both delirium and dementia were more likely to be admitted to long-term care than those with neither condition (adjusted odds ratio 3.18, 95% CI 1.19 to 8.49). Dementia but not delirium predicted worse IADL scores at follow-up. Unadjusted analyses yielded similar results.
Interpretation: For older patients with and without dementia, delirium is an independent predictor of sustained poor cognitive and functional status during the year after a medical admission to hospital.
Figures
References
-
- Lipowski Z. Delirium in geriatric patients. In: Delirium: acute confusional states. New York: Oxford University Press; 1990. p. 413-41.
-
- Levkoff S, Cleary P, Liptzin B, Evans D. Epidemiology of delirium: an overview of research issues and findings. Int Psychogeriatr 1991;3(2):149-67. - PubMed
-
- Francis J, Kapoor WN. Prognosis after hospital discharge of older medical patients with delirium. J Am Geriatr Soc 1992;40:601-6. - PubMed
-
- Murray AM, Levkoff SE, Wetle TT, Beckett L, Cleary PD, Schor JD, et al. Acute delirium and functional decline in the hospitalized elderly patient. J Gerontol 1993;48(5):M181-6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical