

Curative resection for esophageal adenocarcinoma: analysis of 100 en bloc esophagectomies
- PMID: 11573045
- PMCID: PMC1422075
- DOI: 10.1097/00000658-200110000-00011
Curative resection for esophageal adenocarcinoma: analysis of 100 en bloc esophagectomies
Abstract
Objective: To document what can be accomplished with surgical resection done according to the classical principles of surgical oncology.
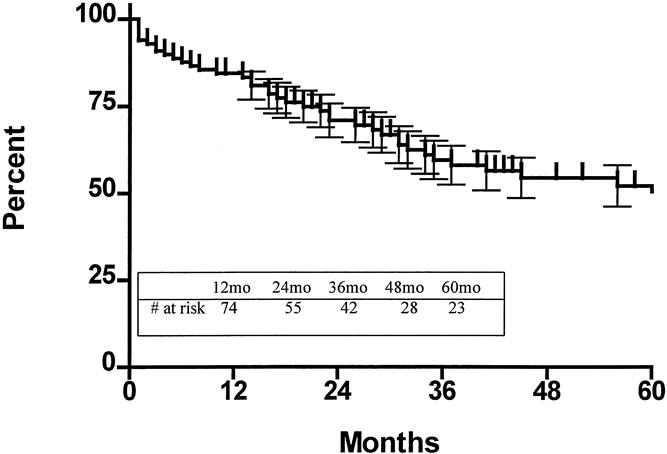
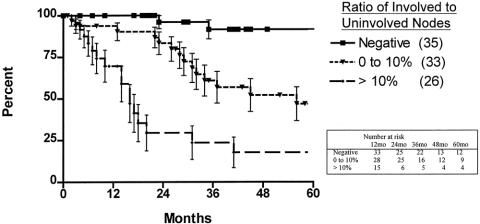
Methods: One hundred consecutive patients underwent en bloc esophagectomy for esophageal adenocarcinoma. No patient received pre- or postoperative chemotherapy or radiation therapy. Tumor depth and number and location of involved lymph nodes were recorded. A lymph node ratio was calculated by dividing the number of involved nodes by the total number removed. Follow-up was complete in all patients. The median follow-up of surviving patients was 40 months, with 23 patients surviving 5 years or more.
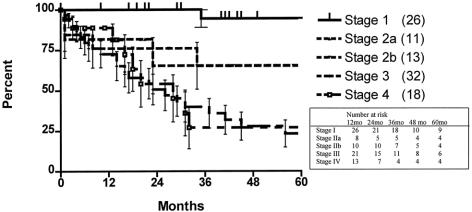
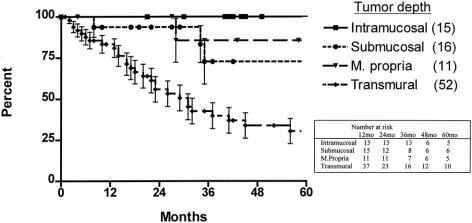
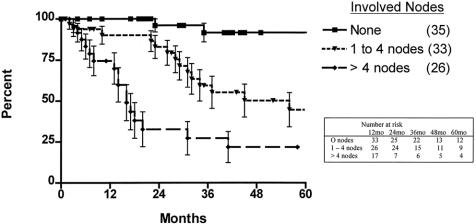
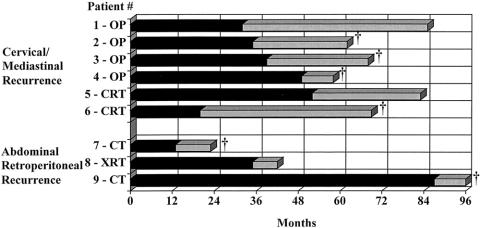
Results: The overall actuarial survival rate at 5 years was 52%. Survival rates by American Joint Commission on Cancer (AJCC) stage were stage 1 (n = 26), 94%; stage 2a (n = 11), 65%; stage 2b (n = 13), 65%; stage 3 (n = 32), 23%; and stage 4 (n = 18), 27%. Sixteen tumors were confined to the mucosa, 16 to the submucosa, and 13 to the muscularis propria, and 55 were transmural. Tumor depth and the number and ratio of involved nodes were predictors of survival. Metastases to celiac (n = 16) or other distant node sites (n = 26) were not associated with decreased survival. Local recurrence was seen in only one patient. Latent nodal recurrence outside the surgical field occurred in 9 patients and systemic metastases in 31. Tumor depth, the number of involved nodes, and the lymph node ratio were important predictors of systemic recurrence. The surgical death rate was 6%.
Conclusion: Long-term survival from adenocarcinoma of the esophagus can be achieved in more than half the patients who undergo en bloc resection. One third of patients with lymph node involvement survived 5 years. Local control is excellent after en bloc resection. The extent of disease associated with tumors confined to the mucosa and submucosa provides justification for more limited and less morbid resections.
Figures
References
-
- Wang HH, Antonioli DA, Goldman H. Comparative features of esophageal and gastric adenocarcinomas: recent changes in type and frequency. Hum Pathol 1986; 17: 482–487. - PubMed
-
- Blot WJ, Devesa SS, Fraumeni JFJ. Continuing climb in rates of esophageal adenocarcinoma: an update [letter]. JAMA 1993; 270: 1320–1321. - PubMed
-
- Sabile J, Rice TW, Goldblum JR, et al. Superficial esophageal carcinoma. Ann Thorac Surg 1995; 60: 896–902. - PubMed
-
- Sampliner RE, Jaffe P. Malignant degeneration of Barrett’s esophagus: the role of laser ablation and photodynamic therapy. Dis Esoph 1995; 8: 104–108.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
