

Early enteral feeding versus "nil by mouth" after gastrointestinal surgery: systematic review and meta-analysis of controlled trials
- PMID: 11588077
- PMCID: PMC57351
- DOI: 10.1136/bmj.323.7316.773
Early enteral feeding versus "nil by mouth" after gastrointestinal surgery: systematic review and meta-analysis of controlled trials
Abstract
Objective: To determine whether a period of starvation (nil by mouth) after gastrointestinal surgery is beneficial in terms of specific outcomes.
Design: Systematic review and meta-analysis of randomised controlled trials comparing any type of enteral feeding started within 24 hours after surgery with nil by mouth management in elective gastrointestinal surgery. Three electronic databases (PubMed, Embase, and the Cochrane controlled trials register) were searched, reference lists checked, and letters requesting details of unpublished trials and data sent to pharmaceutical companies and authors of previous trials.
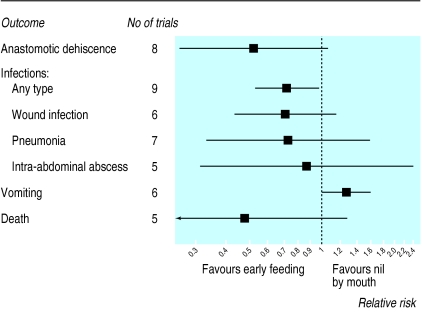
Main outcome measures: Anastomotic dehiscence, infection of any type, wound infection, pneumonia, intra-abdominal abscess, length of hospital stay, and mortality.
Results: Eleven studies with 837 patients met the inclusion criteria. In six studies patients in the intervention group were fed directly into the small bowel and in five studies patients were fed orally. Early feeding reduced the risk of any type of infection (relative risk 0.72, 95% confidence interval 0.54 to 0.98, P=0.036) and the mean length of stay in hospital (number of days reduced by 0.84, 0.36 to 1.33, P=0.001). Risk reductions were also seen for anastomotic dehiscence (0.53, 0.26 to 1.08, P=0.080), wound infection, pneumonia, intra-abdominal abscess, and mortality, but these failed to reach significance (P>0.10). The risk of vomiting was increased among patients fed early (1.27, 1.01 to 1.61, P=0.046).
Conclusions: There seems to be no clear advantage to keeping patients nil by mouth after elective gastrointestinal resection. Early feeding may be of benefit. An adequately powered trial is required to confirm or refute the benefits seen in small trials.
Figures
Comment in
-
Postoperative starvation after gastrointestinal surgery. Early feeding is beneficial.BMJ. 2001 Oct 6;323(7316):761-2. doi: 10.1136/bmj.323.7316.761. BMJ. 2001. PMID: 11588062 Free PMC article. No abstract available.
-
Postoperative starvation after gastrointestinal surgery. Type of intravenous nutrition given in control groups is not indicated.BMJ. 2002 Feb 23;324(7335):481-2. BMJ. 2002. PMID: 11859055 Free PMC article. No abstract available.
-
Postoperative starvation after gastrointestinal surgery. Meta-analysis was not appropriate.BMJ. 2002 Feb 23;324(7335):481-2. BMJ. 2002. PMID: 11863001 No abstract available.
-
Postoperative starvation after gastrointestinal surgery. Anaesthetic technique during gastrointestinal surgery has postoperative effects.BMJ. 2002 Feb 23;324(7335):482. BMJ. 2002. PMID: 11863002 No abstract available.
-
Postoperative starvation after gastrointestinal surgery. Rest in peace, drip and suck.BMJ. 2002 Feb 23;324(7335):481. BMJ. 2002. PMID: 11863003 No abstract available.
References
-
- Catchpole BN. Smooth muscle and the surgeon. Aust N Z J Surg. 1989;59:199–208. - PubMed
-
- Moss G. Maintenance of gastrointestinal function after bowel surgery and immediate enteral full nutrition. II. Clinical experience, with objective demonstration of intestinal absorption and motility. J Parenter Enteral Nutr. 1981;5:215–220. - PubMed
-
- McCarter MD, Gomez ME, Daly JM. Early postoperative enteral feeding following major upper gastrointestinal surgery. J Gastrointest Surg. 1996;1:278–285. - PubMed
-
- Hill GL, Pickford I, Young GA, Schorah CJ, Blackett RL, Burkinshaw L, et al. Malnutrition in surgical patients: an unrecognised problem. Lancet. 1977;i:689–692. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous