

Obstructive sleep apnea and hypertension: from correlative to causative relationship
- PMID: 11588408
- PMCID: PMC8101838
- DOI: 10.1111/j.1524-6175.2001.00491.x
Obstructive sleep apnea and hypertension: from correlative to causative relationship
Abstract
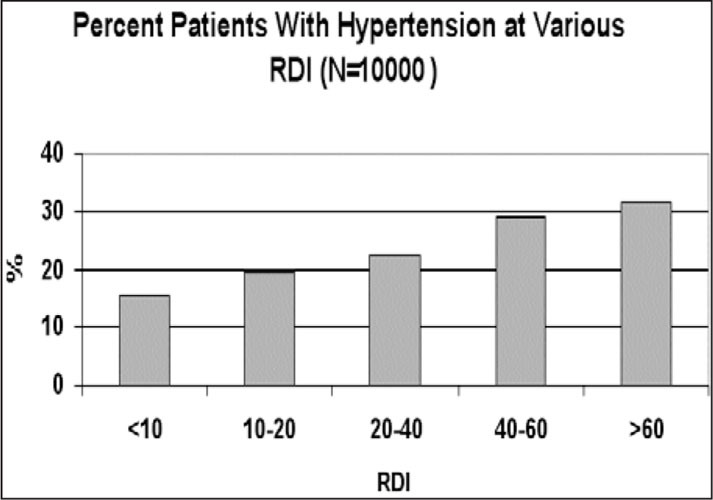
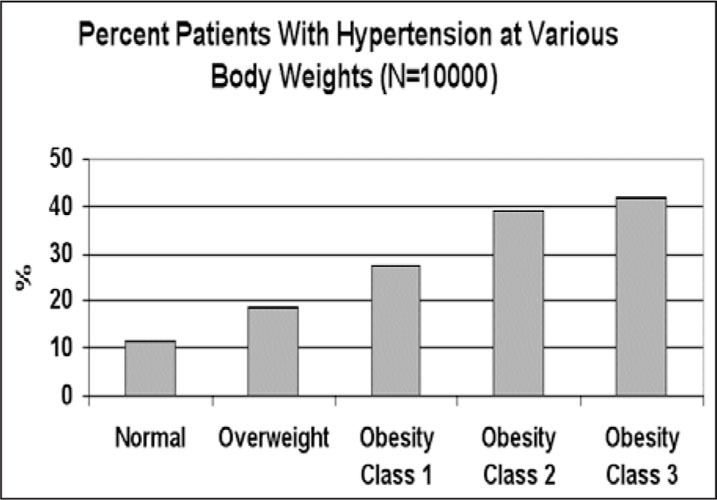
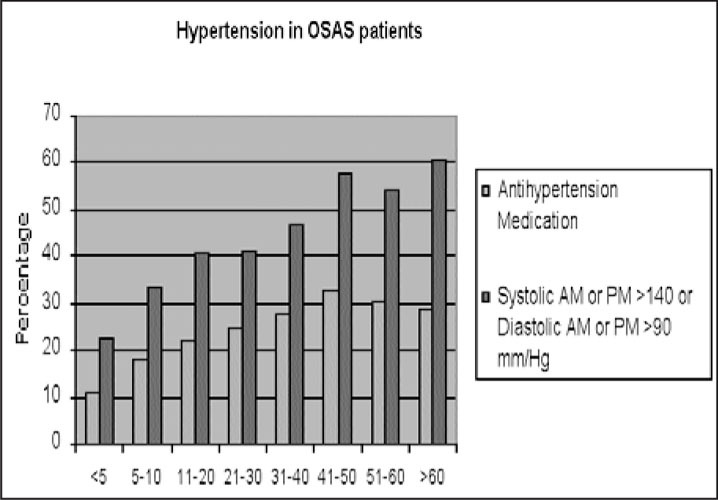
Sleep-disordered breathing, manifested by repetitive episodes of partial or complete cessation of breathing during sleep associated with brief arousal and autonomic activation, is estimated to affect as many as 4% of adult men and 2% of adult women. Studies conducted during the 1980s revealed a strong association between sleep-disordered breathing and hypertension. The results of these early studies, which relied on relatively small samples of patients, have been confirmed in recent years by large-scale epidemiologic studies that are controlled for all possible confounding factors. This paper reviews the evidence suggesting a causative relationship between hypertension and disordered breathing in sleep. The authors discuss the possible underlying mechanisms of the two entities and address the clinical implications of this relationship. They conclude by recommending a proactive approach to the diagnosis of breathing disorders in sleep, in order to prevent the cardiovascular sequelae of this syndrome.
Figures
References
-
- Young T, Palta M, Dempsey J, et al. The occurrence of sleep‐disordered breathing among middle‐aged adults. N Engl J Med. 1993;328:1230–1235. - PubMed
-
- Phillipson EA. Sleep apnea—a major public health problem. N Engl J Med. 1993;328:1271–1273. - PubMed
-
- Lavie P. Incidence of sleep apnea in a presumably healthy working population: a significant relationship with excessive daytime sleepiness. Sleep. 1983;6:312–318. - PubMed
-
- Millman RP, Redline S, Arlisle CC, et al. Daytime hypertension in obstructive sleep apnea. Prevalence and contributing risk factors. Chest. 1991;99:861–866. - PubMed
-
- Silverberg DS, Oksenberg A, Radwan H, et al. Is obstructive sleep apnea a common cause of essential hypertension? Isr J Med Sci. 1995;31:527–535. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
