

Integrating primary medical care with addiction treatment: a randomized controlled trial
- PMID: 11594896
- PMCID: PMC3056510
- DOI: 10.1001/jama.286.14.1715
Integrating primary medical care with addiction treatment: a randomized controlled trial
Abstract
Context: The prevalence of medical disorders is high among substance abuse patients, yet medical services are seldom provided in coordination with substance abuse treatment.
Objective: To examine differences in treatment outcomes and costs between integrated and independent models of medical and substance abuse care as well as the effect of integrated care in a subgroup of patients with substance abuse-related medical conditions (SAMCs).
Design: Randomized controlled trial conducted between April 1997 and December 1998.
Setting and patients: Adult men and women (n = 592) who were admitted to a large health maintenance organization chemical dependency program in Sacramento, Calif.
Interventions: Patients were randomly assigned to receive treatment through an integrated model, in which primary health care was included within the addiction treatment program (n = 285), or an independent treatment-as-usual model, in which primary care and substance abuse treatment were provided separately (n = 307). Both programs were group based and lasted 8 weeks, with 10 months of aftercare available.
Main outcome measures: Abstinence outcomes, treatment utilization, and costs 6 months after randomization.
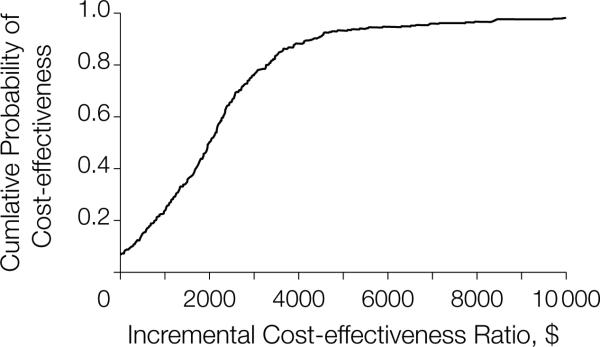
Results: Both groups showed improvement on all drug and alcohol measures. Overall, there were no differences in total abstinence rates between the integrated care and independent care groups (68% vs 63%, P =.18). For patients without SAMCs, there were also no differences in abstinence rates (integrated care, 66% vs independent care, 73%; P =.23) and there was a slight but nonsignificant trend of higher costs for the integrated care group ($367.96 vs $324.09, P =.19). However, patients with SAMCs (n = 341) were more likely to be abstinent in the integrated care group than the independent care group (69% vs 55%, P =.006; odds ratio [OR], 1.90; 95% confidence interval [CI], 1.22-2.97). This was true for both those with medical (OR, 3.38; 95% CI, 1.68-6.80) and psychiatric (OR, 2.10; 95% CI, 1.04-4.25) SAMCs. Patients with SAMCs had a slight but nonsignificant trend of higher costs in the integrated care group ($470.81 vs $427.95, P =.14). The incremental cost-effectiveness ratio per additional abstinent patient with an SAMC in the integrated care group was $1581.
Conclusions: Individuals with SAMCs benefit from integrated medical and substance abuse treatment, and such an approach can be cost-effective. These findings are relevant given the high prevalence and cost of medical conditions among substance abuse patients, new developments in medications for addiction, and recent legislation on parity of substance abuse with other medical benefits.
Figures

Comment in
-
Generalist physicians and addiction care: from turfing to sharing the turf.JAMA. 2001 Oct 10;286(14):1764-5. doi: 10.1001/jama.286.14.1764. JAMA. 2001. PMID: 11594904 No abstract available.
References
-
- Stein MD. Medical consequences of substance abuse. Psychiatr Clin North Am. 1999;22:351–370. - PubMed
-
- Chou SP, Grant BF, Dawson DA. Medical consequences of alcohol consumption—United States, 1992. Alcohol Clin Exp Res. 1996;20:1423–1429. - PubMed
-
- Sikkink J, Fleming M. Adverse health effects and medical complications of alcohol, nicotine, and drug use. In: Fleming MF, Barry KL, editors. Addictive Disorders. Mosby–Year Book; St Louis, Mo: 1991. pp. 145–168.
-
- Heischober B, Miller MA. Methamphetamine abuse in California. In: Miller MA, Kozel NJ, editors. Methamphetamine Abuse: Epidemiologic Issues and Implications. US National Institute on Drug Abuse; Rockville, Md: 1991. pp. 60–71.
-
- Weisner C. Chronic alcohol and drug abuse. In: Newcomer RJ, Benjamin AE, editors. Indicators of Chronic Health Conditions: Monitoring Community-Level Delivery Systems. Johns Hopkins University Press; Baltimore, Md: 1997. pp. 260–301.
