

Incidence and prognostic significance of atrial fibrillation in acute myocardial infarction: the GISSI-3 data
- PMID: 11602545
- PMCID: PMC1729969
- DOI: 10.1136/heart.86.5.527
Incidence and prognostic significance of atrial fibrillation in acute myocardial infarction: the GISSI-3 data
Abstract
Background: Atrial fibrillation is the most common supraventricular arrhythmia in patients with acute myocardial infarction. Recent advances in pharmacological treatment of myocardial infarction may have changed the impact of this arrhythmia.
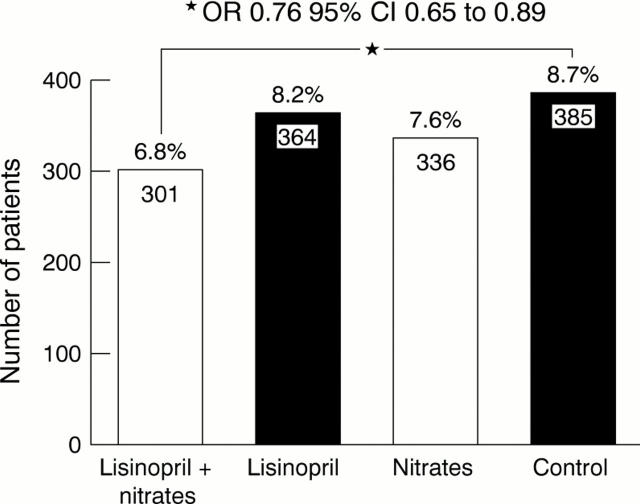
Objective: To assess the incidence and prognosis of atrial fibrillation complicating myocardial infarction in a large population of patients receiving optimal treatment, including angiotensin converting enzyme (ACE) inhibitors.
Methods: Data were derived from the GISSI-3 trial, which included 17 944 patients within the first 24 hours after acute myocardial infarction. Atrial fibrillation was recorded during the hospital stay, and follow up visits were planned at six weeks and six months. Survival of the patients at four years was assessed through census offices.
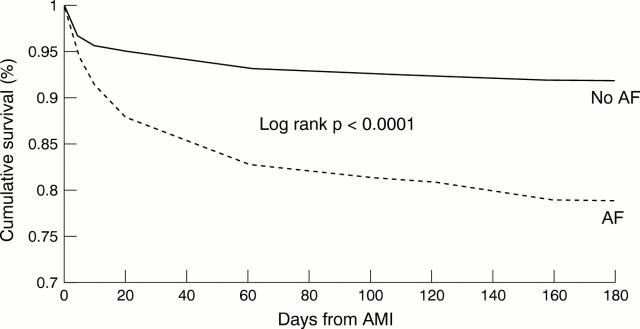
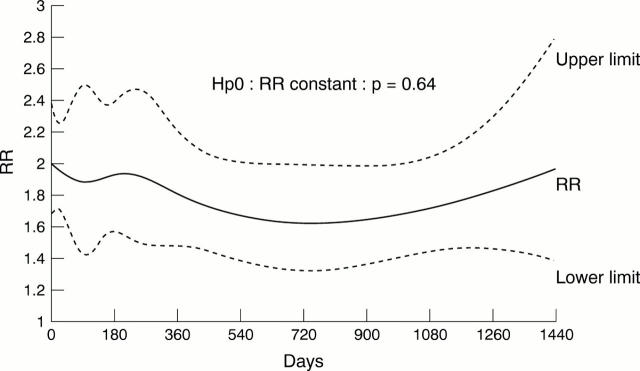
Results: The incidence of in-hospital atrial fibrillation or flutter was 7.8%. Atrial fibrillation was associated with indicators of a worse prognosis (age > 70 years, female sex, higher Killip class, previous myocardial infarction, treated hypertension, high systolic blood pressure at entry, insulin dependent diabetes, signs or symptoms of heart failure) and with some adverse clinical events (reinfarction, sustained ventricular tachycardia, ventricular fibrillation). After adjustment for other prognostic factors, atrial fibrillation remained an independent predictor of increased in-hospital mortality: 12.6% v 5%, adjusted relative risk (RR) 1.98, 95% confidence interval (CI) 1.67 to 2.34. Data on long term mortality (four years after acute myocardial infarction) confirmed the persistent negative influence of atrial fibrillation (RR 1.78, 95% CI 1.60 to 1.99).
Conclusions: Atrial fibrillation is an indicator of worse prognosis after acute myocardial infarction, both in the short term and in the long term, even in an unselected population.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous