

Curtailing unnecessary vancomycin usage in a hospital with high rates of methicillin resistant Staphylococcus aureus infections
- PMID: 11678786
- PMCID: PMC2014574
- DOI: 10.1046/j.0306-5251.2001.01455.x
Curtailing unnecessary vancomycin usage in a hospital with high rates of methicillin resistant Staphylococcus aureus infections
Abstract
Aims: To implement and monitor the effectiveness of a strategy to curb unnecessary use of vancomycin and teicoplanin for inpatients in a teaching hospital/tertiary referral centre where 33% of S. aureus isolates (72% from ICU patients) were methicillin resistant.
Methods: A sample of 182 vancomycin/teicoplanin inpatient prescriptions surveyed, revealed that only 31 (17%) conformed with Centre for Disease Control (CDC) guidelines. Following education (ward-rounds, bulletins) on appropriate CDC based guidelines for prescribing glycopeptides directed at relevant clinicians, 'Immediate Concurrent Feedback' (ICF) was gradually deployed throughout the hospital. This entailed review of respective inpatient records on the next working day. If the indication was deemed not to conform with our guidelines, the prescriber was issued a memo (copied to the supervising doctor). Each memo detailed the 'errant' incident, listed appropriate indications and explicitly advised desisting from such prescribing and suggested alternative therapy if necessary. Corresponding glycopeptide usage data for our hospital and others in Hong Kong were retrieved and analysed as were samples of records of our inpatients with staphylococcal septicaemia (pre and during ICF).
Results: Compared with baseline values, during 2 years of ICF, inpatient prescribing of vancomycin and teicoplanin deemed to conform increased to 71% (773/1086); difference 54% (P < 0.0001, 95% CIs 47-62%). Corresponding average monthly usage (DDDs/1000 admissions) decreased from 76 (pre-ICF) to 45; mean difference 31 (P < 0.0001, 95% CIs 24, 38). Mortality from staphylococcal bacteraemia remained unchanged. No comparable changes in glycopeptide usage ensued in comparator hospitals.
Conclusions: ICF can be used safely to curb irrational overuse of vancomycin and teicoplanin in a hospital with high methicillin resistant S. aureus infection rates.
Figures
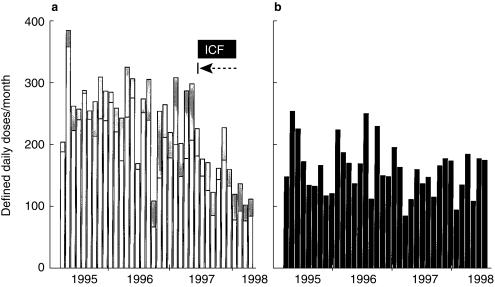
 ), where the ICF programme was first implemented from August 1997. (b) Other departments in the hospital (▪), where the ICF programme was only introduced gradually over several months starting in January 1998. |→–– represents initiation of immediate concurrent feedback (ICF).
), where the ICF programme was first implemented from August 1997. (b) Other departments in the hospital (▪), where the ICF programme was only introduced gradually over several months starting in January 1998. |→–– represents initiation of immediate concurrent feedback (ICF).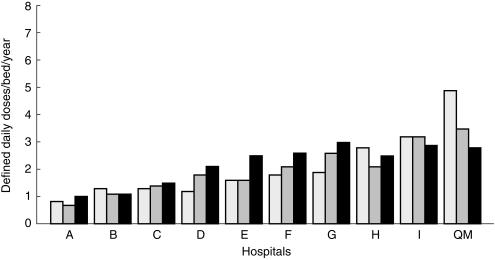
References
-
- Recommendations for preventing the spread of vancomycin resistance. Suppl to MMWR. 1995. pp. 1–13. - PubMed
-
- Keane WF, Alexander SR, Bailie GR, et al. Peritonial dialysis – related peritonitis treatment recommendations: 1996 Update. Perit Dial Int. 1996;16:557–573. - PubMed
-
- Anglim AM, Klym B, Byers KE, et al. Effect of a vancomycin restriction policy on ordering practices during an outbreak of vancomycin-resistant Enterococcus faecium. Arch Intern Med. 1997;157:1132–1136. - PubMed
-
- Lipsky BA, Baker CA, McDonald LL, et al. Improving the appropriateness of vancomycin use by sequential intervention. Am J Infect Control. 1999;27:84–90. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
