

Statins for primary prevention: at what coronary risk is safety assured?
- PMID: 11678788
- PMCID: PMC2014585
- DOI: 10.1046/j.0306-5251.2001.01478.x
Statins for primary prevention: at what coronary risk is safety assured?
Abstract
Aims: Increasingly HMG CoA reductase inhibitors (statins) are being used for primary prevention of vascular disease in patients with a raised cholesterol but at low absolute risk of coronary heart disease (CHD). This study uses clinical trial results to explore the limits of absolute safety for statin use in such patients.
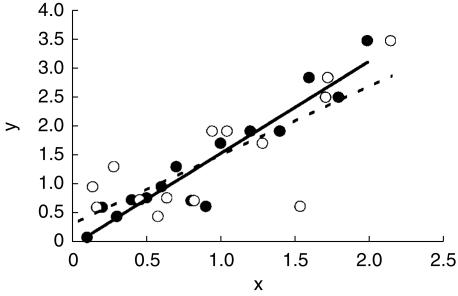
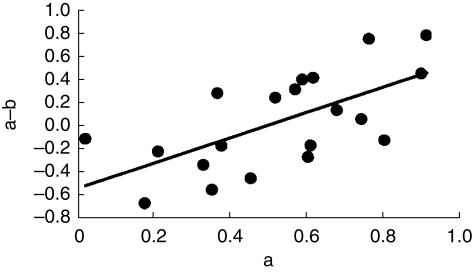
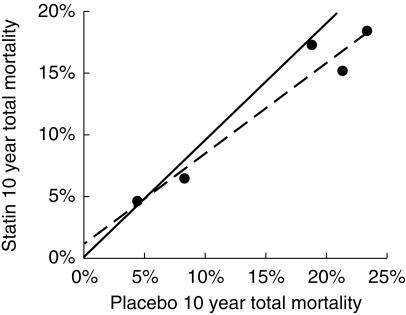
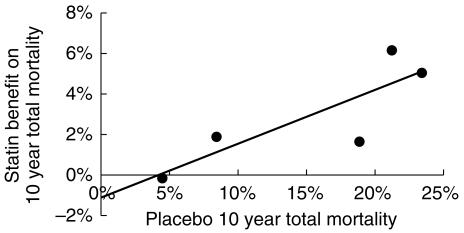
Methods: The major placebo controlled statin outcome trials were identified by automated and manual literature searches. Principal results including all cause mortality in placebo and intervention groups and baseline values of standard coronary risk factors were abstracted for each trial. For the trials identified the reduction in overall mortality with statin treatment for each study was regressed against the underlying CHD risk of the population recruited into that trial using a statistically robust method.
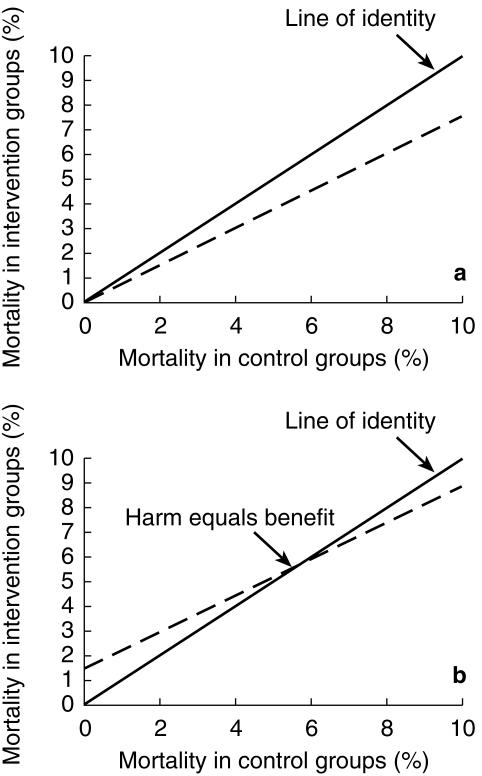
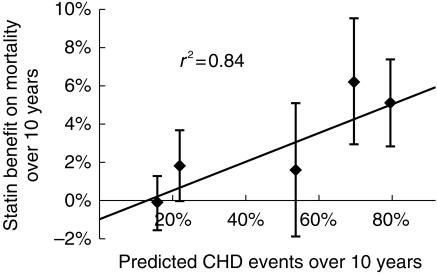
Results: The regression line describing the relationship between mortality benefit and risk suggests that statin use could be associated with an increase in mortality of 1% in 10 years. This would be sufficiently large to negate statin's beneficial effect on CHD mortality in patients with a CHD event risk less than 13% over 10 years.
Conclusions: Absolute safety of statins has not been demonstrated for patients at low risk of CHD. Patients absolute risk of CHD should be calculated before starting statin treatment for primary prevention. Extensions of such treatment to low risk patients should await further evidence of safety.
Figures
References
-
- Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S) Lancet. 1994. pp. 439–446. - PubMed
-
- The Lipid Research Clinics Coronary Prevention Trial results I. Reduction in coronary heart disease. JAMA. 1984;251:351–364. - PubMed
-
- Gould AL, Rossouw JE, Santanello NC, et al. Cholesterol reduction yields clinical benefit. A new look at old data. Circulation. 1995;91:2274–2282. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
