

Randomised trials of secondary prevention programmes in coronary heart disease: systematic review
- PMID: 11679383
- PMCID: PMC58658
- DOI: 10.1136/bmj.323.7319.957
Randomised trials of secondary prevention programmes in coronary heart disease: systematic review
Abstract
Objective: To determine whether multidisciplinary disease management programmes for patients with coronary heart disease improve processes of care and reduce morbidity and mortality.
Data sources: Randomised clinical trials of disease management programmes in patients with coronary heart disease were identified by searching Medline 1966-2000, Embase 1980-99, CINAHL 1982-99, SIGLE 1980-99, the Cochrane controlled trial register, the Cochrane effective practice and organisation of care study register, and bibliographies of published studies.
Data extraction: Studies were selected and data were extracted independently by two investigators, and summary risk ratios were calculated by using both the random effects model and the fixed effects model.
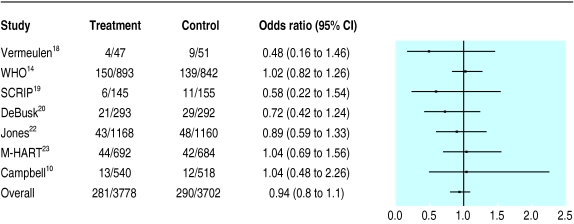
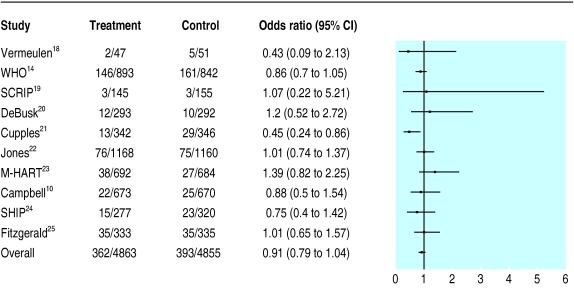
Data synthesis: A total of 12 trials (9803 patients with coronary heart disease) were identified. Disease management programmes had positive impacts on processes of care. Patients randomised to these programmes were more likely to be prescribed efficacious drugs (risk ratio 2.14 (95% confidence interval 1.92 to 2.38) for lipid lowering drugs, 1.19 (1.07 to 1.32) for beta blockers, and 1.07 (1.03 to 1.11) for antiplatelet agents). Five out of seven trials evaluating risk factor profiles showed significantly greater improvements with these programmes in comparison with usual care (with effect sizes in the moderate range). Summary risk ratios were 0.91 (0.79 to 1.04) for all cause mortality, 0.94 (0.80 to 1.10) for recurrent myocardial infarction, and 0.84 (0.76 to 0.94) for admission to hospital. Five of the eight trials evaluating quality of life or functional status reported better outcomes in the intervention arms. Only three of these trials reported the costs of the intervention-the interventions were cost saving in two cases.
Conclusions: Disease management programmes improve processes of care, reduce admissions to hospital, and enhance quality of life or functional status in patients with coronary heart disease. The programmes' impact on survival and recurrent infarctions, their cost effectiveness, and the optimal mix of components remain uncertain.
Figures
Comment in
-
Review: multidisciplinary CHD management programs improve the process of care and reduce hospitalizations.ACP J Club. 2002 Mar-Apr;136(2):73. ACP J Club. 2002. PMID: 11874298 No abstract available.
-
Secondary prevention of coronary heart disease. Ill defined inclusion criteria resulted in missed trials.BMJ. 2002 Mar 9;324(7337):611. BMJ. 2002. PMID: 11884335 Free PMC article. No abstract available.
-
Secondary prevention of coronary heart disease. Secondary prevention programmes may reduce overall mortality in high risk patients.BMJ. 2002 Mar 9;324(7337):611. BMJ. 2002. PMID: 11887885 No abstract available.
-
Secondary prevention of coronary heart disease. Improved outcomes need to be defined.BMJ. 2002 Mar 9;324(7337):611-2. BMJ. 2002. PMID: 11887886 No abstract available.
-
Review: multidisciplinary disease management programmes do not reduce death or recurrent myocardial infarction but reduce admission to hospital.Evid Based Nurs. 2002 Apr;5(2):54. doi: 10.1136/ebn.5.2.54. Evid Based Nurs. 2002. PMID: 11995657 No abstract available.
References
-
- EUROASPIRE I and II Group. Clinical reality of coronary prevention guidelines: a comparison of EUROASPIRE I and II in nine countries. Lancet. 2001;357:995–1001. - PubMed
-
- Greenland P. Closing the treatment gap: in the community and at hospital discharge. Am J Med. 1996;101(suppl 4A):76–78S. - PubMed
-
- Cohen JD. ABCs of secondary prevention of CHD: easier said than done. Lancet. 2001;357:972–973. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources