

A meta-analysis of the effects of cigarette smoking on bone mineral density
- PMID: 11683532
- PMCID: PMC5352985
- DOI: 10.1007/BF02390832
A meta-analysis of the effects of cigarette smoking on bone mineral density
Abstract
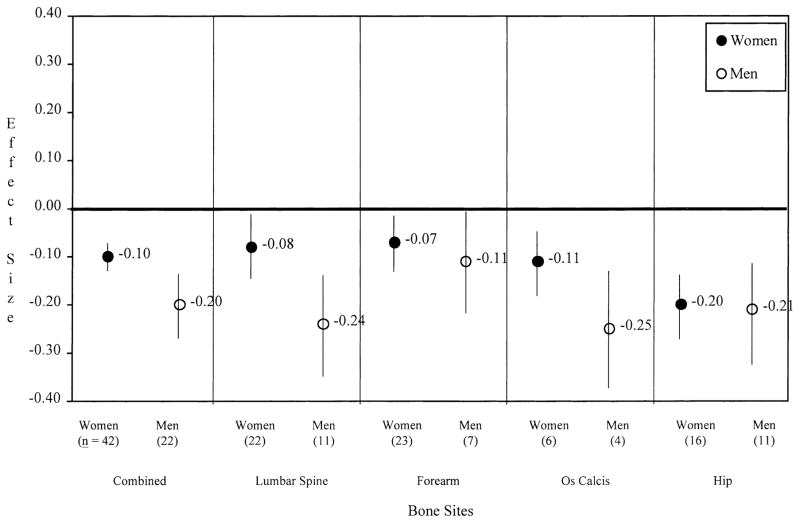
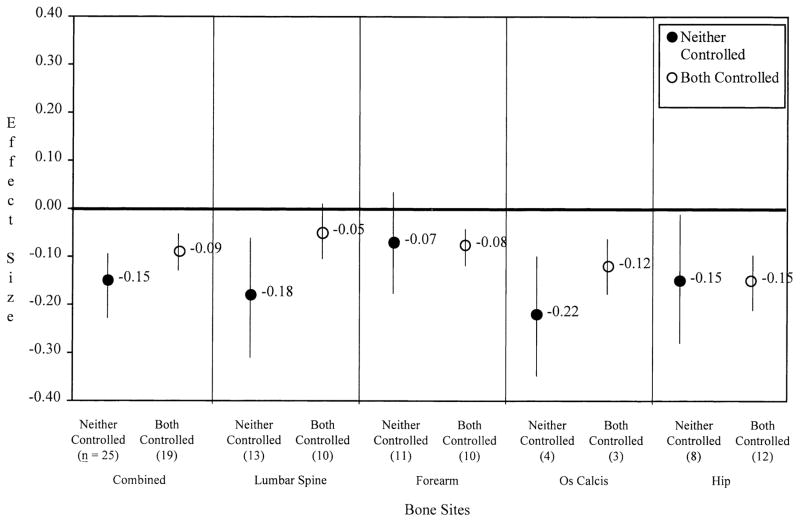
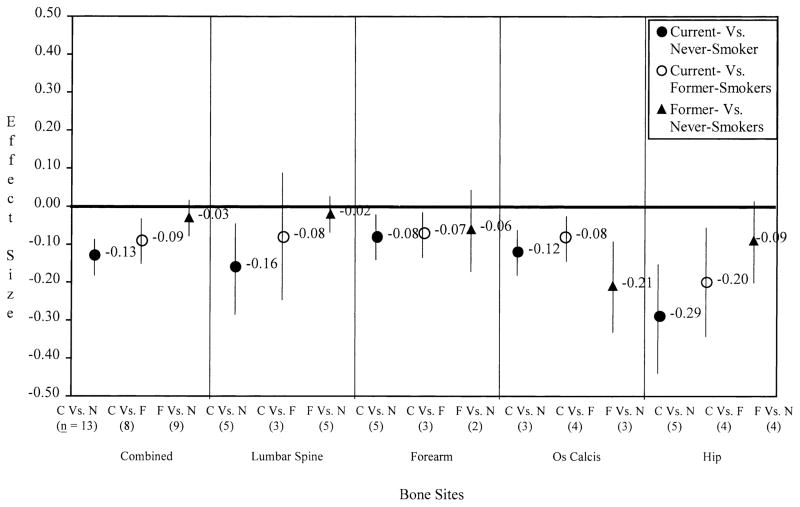
To determine the magnitude and mediators of the association between cigarette smoking and bone mass in the epidemiologic literature we reviewed articles, published abstracts, and conference proceedings, identified through MEDLINE, psychological abstracts, conference proceedings, and article bibliographies. We studied cross-sectional and prospective human studies that provided a quantitative measure of bone mass (X-ray, absorptiometry, or computed tomography) as a function of cigarette smoking exposure. Effects were expressed as pooled standardized mean differences for categorical comparisons (e.g., bone mass in current versus nonsmokers), and as pooled correlation coefficients for continuous comparisons (e.g., correlation of bone mass and pack-years of smoking). Effects were derived for combined bone sites (all bone sites pooled within each study) and four specific sites (hip, lumbar spine, forearm, and os calcis), and were examined overall and as a function of subject and methodologic characteristics (gender, age, body weight, menopausal status, health status). Data were pooled across 86 studies, enrolling 40,753 subjects. Smokers had significantly reduced bone mass compared with nonsmokers (never and former smokers) at all bone sites, averaging a one-tenth standard deviation (SD) deficit for combined sites. Deficits were especially pronounced at the hip, where the bone mass of current smokers was one-third of a SD less than that of never smokers. Overall, effects were greatest in men and in the elderly, and were dose-dependent. In prospective studies, smokers had greater rates of bone loss over time compared with nonsmokers. Bone mass differences remained significant after controlling for age and body weight differences between the two groups. Absolute effect sizes at most bone sites were greatest for current smokers compared with never smokers, intermediate for current smokers compared with former smokers, and lowest for former smokers compared with never smokers, suggesting that smoking cessation may have a positive influence on bone mass. Based on these data, it is estimated that smoking increases the lifetime risk of developing a vertebral fracture by 13% in women and 32% in men. At the hip, smoking is estimated to increase lifetime fracture risk by 31% in women and 40% in men. It appears that smoking has an independent, dose-dependent effect on bone loss, which increases fracture risk, and may be partially reversed by smoking cessation. Given the public health implications of smoking on bone health, it is important that this information be incorporated into smoking prevention and cessation efforts.
Figures
References
References (asterisked articles in the bibliography were included in the meta-analysis)
-
- Cooper C, Wickham C. Cigarette smoking and the risk of age-related fractures. In: Wald N, Baron J, editors. Smoking and hormone-related disorders. Oxford University Press; Oxford: 1990. pp. 93–100.
-
- Daniel M, Martin AD, Drinkwater DT. Cigarette smoking, steroid hormones, and bone mineral density in young women. Calcif Tissue Int. 1992;50:300–305. - PubMed
-
- Johnell O, Nilsson BE. Life-style and bone mineral mass in perimenopausal women. Calcif Tissue Int. 1984;36:354–356. - PubMed
Additional Studies Included in the Meta-Analysis
-
- Bendavid EJ, Shan J, Barrett-Connor E. Factors associated with bone mineral density in middle-aged men. J Bone Miner Res. 1996;11:1185–1190. - PubMed
-
- Cheng S, Suominen H, Rantanen T, Parkatti T, Heikkinen E. Bone mineral density and physical activity in 50–60-year-old women. Bone Miner. 1991;12:123–132. - PubMed
-
- Cooper C, Cawley M, Bhalla A, Egger P, Ring F, Morton L, Barker D. Childhood growth, physical activity, and peak bone mass in women. J Bone Miner Res. 1995;10:940–947. - PubMed
-
- Falch JA, Sandvik L, Van Beresteijn ECH. Development and evaluation of an index to predict early postmenopausal bone loss. Bone. 1992;13:337–341. - PubMed
-
- Hall ML, Heavens J, Cullum ID, Ell PJ. The range of bone density in normal British women. Br J Radiol. 1990;63:266–269. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
