

Endoscopic surveillance of columnar-lined esophagus: frequency of intestinal metaplasia detection and impact of antireflux surgery
- PMID: 11685024
- PMCID: PMC1422085
- DOI: 10.1097/00000658-200111000-00006
Endoscopic surveillance of columnar-lined esophagus: frequency of intestinal metaplasia detection and impact of antireflux surgery
Abstract
Objective: To quantify the occurrence of intestinal metaplasia in columnar-lined esophagus (CLE) during endoscopic surveillance and to evaluate the impact of antireflux surgery on the development of intestinal metaplasia.
Summary background data: The malignant potential in segments of CLE is mainly restricted to those containing intestinal metaplasia. Patients with segments of CLE in which no intestinal metaplasia can be detected are rarely enrolled in a surveillance program but may still be at increased risk of developing esophageal adenocarcinoma because intestinal metaplasia may be missed or may develop with time.
Methods: The occurrence of intestinal metaplasia on biopsy samples was determined on repeated endoscopies in 177 patients enrolled in a surveillance program for CLE. The incidence of intestinal metaplasia in patients with no evidence of intestinal metaplasia on the two first endoscopies was evaluated on the subsequent endoscopies and compared in patients with medically and surgically treated gastroesophageal reflux disease.
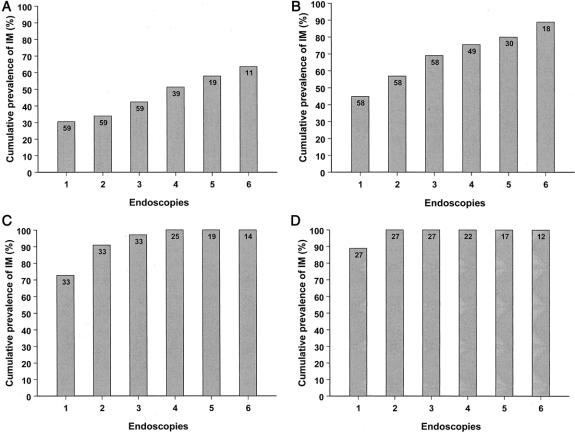
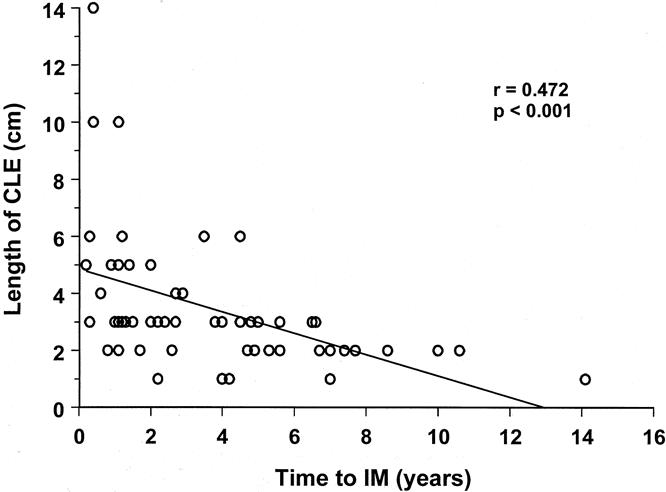
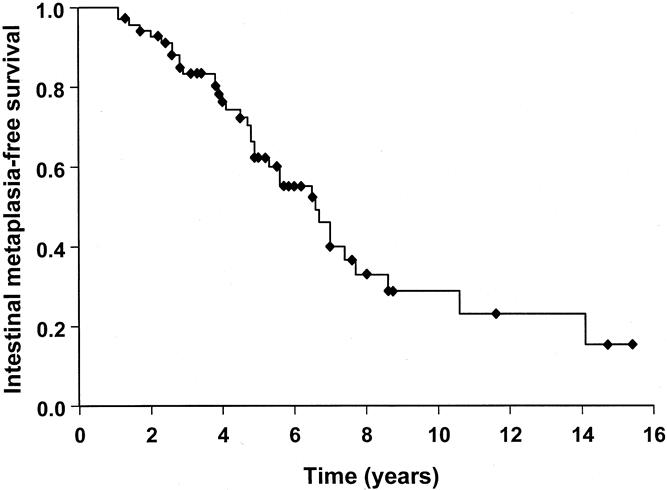
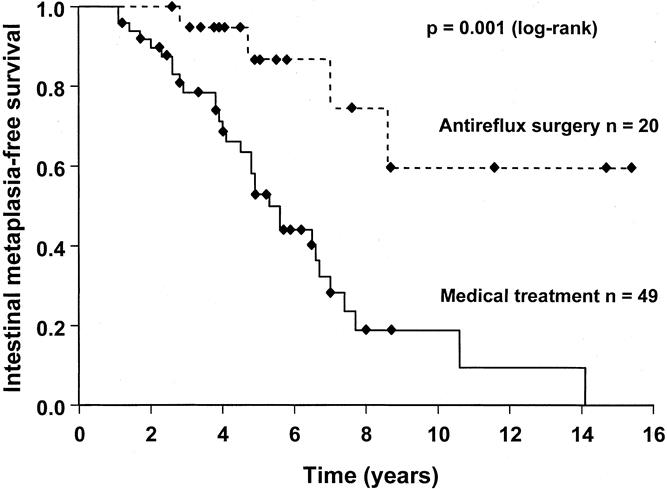
Results: Intestinal metaplasia was found in 53% of the patients (94/177) on their first surveillance endoscopy and was more prevalent in long segments of CLE. The prevalence of intestinal metaplasia increased markedly with increasing number of surveillance endoscopies. Intestinal metaplasia tended to be detected early in patients with long segments of CLE; in patients with shorter segments, intestinal metaplasia was also detected late in the course of endoscopic surveillance. Patients with surgically treated reflux disease were 10.3 times less likely to develop intestinal metaplasia compared with a group receiving standard medical therapy.
Conclusion: Biopsy samples from a single endoscopy, despite an adequate biopsy protocol, are insufficient to rule out the presence of intestinal metaplasia. Patients in whom biopsy specimens from a segment of CLE show no intestinal metaplasia have a significant risk of having undetected intestinal metaplasia or of developing intestinal metaplasia with time. Sampling error is probably the reason for the absence of intestinal metaplasia in segments of CLE longer than 4 cm, whereas development of intestinal metaplasia is common in patients with shorter segments of CLE. Antireflux surgery protects against the development of intestinal metaplasia, possibly by better control of reflux of gastric contents.
Figures
Similar articles
-
Impact of antireflux operation on columnar-lined esophagus.J Am Coll Surg. 2003 Jan;196(1):60-7. doi: 10.1016/s1072-7515(02)01502-8. J Am Coll Surg. 2003. PMID: 12517552 Review.
-
Prevalence and predictors of columnar lined esophagus in gastroesophageal reflux disease (GERD) patients undergoing upper endoscopy.Am J Gastroenterol. 2012 Nov;107(11):1655-61. doi: 10.1038/ajg.2012.299. Epub 2012 Oct 2. Am J Gastroenterol. 2012. PMID: 23032983
-
Determinants of intestinal metaplasia within the columnar-lined esophagus.Arch Surg. 2000 Jun;135(6):651-5; discussion 655-6. doi: 10.1001/archsurg.135.6.651. Arch Surg. 2000. PMID: 10843360
-
Prevalence of intestinal metaplasia according to the length of the specialized columnar epithelium lining the distal esophagus in patients with gastroesophageal reflux.Dis Esophagus. 2003;16(1):24-8. doi: 10.1046/j.1442-2050.2003.00284.x. Dis Esophagus. 2003. PMID: 12581250
-
Short and ultrashort Barrett's esophagus--what does it mean?Semin Gastrointest Dis. 1997 Apr;8(2):59-67. Semin Gastrointest Dis. 1997. PMID: 9109693 Review.
Cited by
-
Videoendoscopy and histopathology of the esophagogastric junction in patients with gastroesophageal reflux disease.Wien Klin Wochenschr. 2007;119(9-10):283-90. doi: 10.1007/s00508-007-0786-3. Wien Klin Wochenschr. 2007. PMID: 17571232
-
The interplay between Helicobacter pylori, gastro-oesophageal reflux disease, and intestinal metaplasia.Gut. 2005 Mar;54 Suppl 1(Suppl 1):i13-20. doi: 10.1136/gut.2004.041533. Gut. 2005. PMID: 15711003 Free PMC article. Review.
-
Histologic Features Associated With Columnar-lined Esophagus in Distal Esophageal and Gastroesophageal Junction (GEJ) Biopsies From GERD Patients: A Community-based Population Study.Am J Surg Pathol. 2016 Jun;40(6):827-35. doi: 10.1097/PAS.0000000000000623. Am J Surg Pathol. 2016. PMID: 26927889 Free PMC article.
-
Histopathology of the endoscopic esophagogastric junction in patients with gastroesophageal reflux disease.Wien Klin Wochenschr. 2008;120(11-12):350-9. doi: 10.1007/s00508-008-0997-2. Wien Klin Wochenschr. 2008. PMID: 18709523
-
Efficacy of Nissen Sleeve Gastrectomy on Mid-term Barrett's Esophagus Regression.Obes Surg. 2024 Feb;34(2):382-388. doi: 10.1007/s11695-023-07034-y. Epub 2024 Jan 6. Obes Surg. 2024. PMID: 38183594
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
