

Antibacterial prescribing and antibacterial resistance in English general practice: cross sectional study
- PMID: 11691763
- PMCID: PMC59384
- DOI: 10.1136/bmj.323.7320.1037
Antibacterial prescribing and antibacterial resistance in English general practice: cross sectional study
Abstract
Objective: To quantify the relation between community based antibacterial prescribing and antibacterial resistance in community acquired disease.
Design: Cross sectional study of antibacterial prescribing and antibacterial resistance of routine isolates within individual practices and primary care groups.
Setting: 405 general practices (38 groups) in south west and north west England.
Main outcome measures: Correlation between antibacterial prescribing and resistance for urinary coliforms and Streptococcus pneumoniae.
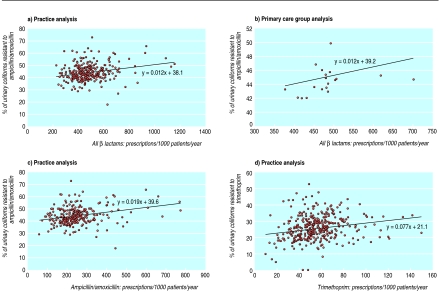
Results: Antibacterial resistance in urinary coliform isolates is common but the correlation with prescribing rates was relatively low for individual practices (ampicillin and amoxicillin r(s)=0.20, P=0.001; trimethoprim r(s)=0.24, P=0.0001) and primary care groups (ampicillin and amoxicillin r(s)=0.44, P=0.05; trimethoprim r(s)=0.31, P=0.09). Regression coefficients were also low; a practice prescribing 20% less ampicillin and amoxicillin than average would have about 1% fewer resistant isolates (0.94/100; 95% confidence interval 0.02 to 1.85). Resistance of S pneumoniae to both penicillin and erythromycin remains uncommon, and no clear relation with prescribing was found.
Conclusions: Routine microbiological isolates should not be used for surveillance of antibacterial resistance in the community or for monitoring the outcome of any change in antibacterial prescribing by general practitioners. Trying to reduce the overall level of antibiotic prescribing in UK general practice may not be the most effective strategy for reducing resistance in the community.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical