

Immunophenotypic analysis of the TCR-Vbeta repertoire in 98 persistent expansions of CD3(+)/TCR-alphabeta(+) large granular lymphocytes: utility in assessing clonality and insights into the pathogenesis of the disease
- PMID: 11696446
- PMCID: PMC1867049
- DOI: 10.1016/s0002-9440(10)63032-5
Immunophenotypic analysis of the TCR-Vbeta repertoire in 98 persistent expansions of CD3(+)/TCR-alphabeta(+) large granular lymphocytes: utility in assessing clonality and insights into the pathogenesis of the disease
Abstract
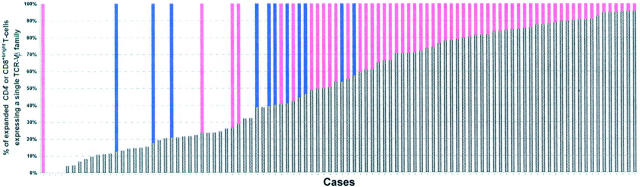
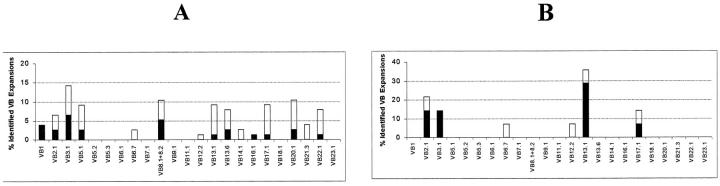
At present, a major challenge in the initial diagnosis of leukemia of large granular lymphocytes (LGLs) is to establish the clonal nature of the expanded population. In the present study we have analyzed by flow cytometry immunophenotyping the TCR-Vbeta repertoire of 98 consecutive cases of persistent expansions of CD4(+) or CD8(+bright) CD3(+)/TCR-alphabeta(+) LGLs and compared the results with those obtained in molecular studies of TCR-beta gene rearrangements. Fifty-eight cases were considered to be monoclonal in molecular studies whereas in the remaining 40 cases there was no evidence for monoclonality (11 cases were considered oligoclonal and 29 polyclonal). The TCR-Vbeta repertoire was biased to the preferential use of one or more TCR-Vbeta families in 96% of cases, a total of 124 TCR-Vbeta expansions being diagnosed: one TCR-Vbeta expansion in 71 cases and two or more TCR-Vbeta expansions in 23 cases. The highest TCR-Vbeta expansion observed in each case was higher among monoclonal (74 +/- 19%) as compared to nonmonoclonal cases (24 +/- 14%) (P = 0.001), as did the fraction of LGLs that exhibited a TCR-Vbeta-restricted pattern (86 +/- 16% and 42 +/- 23%, respectively; P = 0.0001); by contrast, the proportion of cases displaying more than one TCR-Vbeta expansion was higher in the latter group: 7% versus 48%, respectively (P = 0.001). Results obtained in oligoclonal cases were intermediate between those obtained in polyclonal and monoclonal cases and similar results were observed for CD4(+) as for CD8(+bright) T-cell expansions. TCR-Vbeta families expressed in CD8(+bright) T-cell-LGL proliferations showed a pattern of distribution that mimics the frequency at which the individual TCR-Vbeta families are represented in normal peripheral blood T cells. Assuming that a given proliferation of LGLs is monoclonal whenever there is an expansion of a given TCR-Vbeta family of at least 40% of the total CD4(+) or CD8(+bright) T-cell compartment, we were able to predict clonality with a sensitivity of 93% and a specificity of 80%. By increasing the cut-off value to 60%, sensitivity and specificity were of 81% and 100%. In summary, our results suggest that flow cytometry immunophenotypic analysis of the TCR-Vbeta repertoire is a powerful screening tool for the assessment of T-cell clonality in persistent expansions of TCR-alphabeta(+) LGLs.
Figures
References
-
- Loughran TP: Clonal diseases of large granular lymphocytes. Blood 1993, 82:1-14 - PubMed
-
- Scott CS, Richard SJ: Classification of large granular lymphocyte (LGL) and NK-associated (NKa) disorders. Blood Rev 1992, 6:220-233 - PubMed
-
- Semenzato G, Pandolfi F, Chisesi T, De Rossi G, Pizzolo G, Zambello R, Trentim L, Agostini C, Dini E, Vespignani M, Cafaro A, Pasqualetti D, Giubellino MC, Migone N, Foa R: The lymphoproliferative disease of granular lymphocytes. A heterogeneous disease ranging from indolent to aggressive conditions. Cancer 1987, 60:2971-2978 - PubMed
-
- Scott CS, Richards SJ, Sivakumaran M, Short M, Child JÁ, Hunt KM, McEvoy M, Steed AJ, Balfour IC, Parapia LA: Transient and persistent expansions of large granular lymphocytes (LGL) and NK associated (NKs) cells: the Yorkshire Leukaemia Group Study. Br J Haematol 1993, 83:505-517 - PubMed
-
- Semenzato G, Pizzoto G, Rannunci A, Agostini C, Chilosi M, Quinti I, De Sanctis G, Vercelli B, Pandolfi F: Abnormal expansion of polyclonal large to small size granular lymphocytes: reactive or neoplastic process? Blood 1984, 63:1271-1277 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
