

Interleukin 16 expression and phenotype of interleukin 16 producing cells in Crohn's disease
- PMID: 11709514
- PMCID: PMC1728558
- DOI: 10.1136/gut.49.6.795
Interleukin 16 expression and phenotype of interleukin 16 producing cells in Crohn's disease
Abstract
Background: The mechanisms involved in the initiation and maintenance of Crohn's disease are poorly understood. Previous studies have demonstrated an increased number of infiltrating CD4+ T cells within the inflammatory affected bowel wall in Crohn's disease. Novel therapy approaches using anti-CD4 antibodies are thought to be effective in Crohn's disease.
Aims: Interleukin 16 (IL-16) has been characterised as a chemokine with selective chemoattraction for CD4+ inflammatory T cells. In this study, cellular expression of IL-16 in Crohn's disease and ulcerative colitis was investigated.
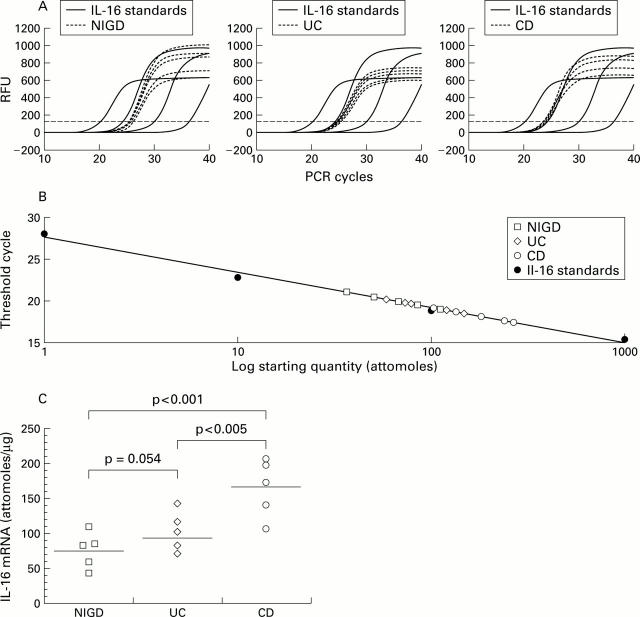
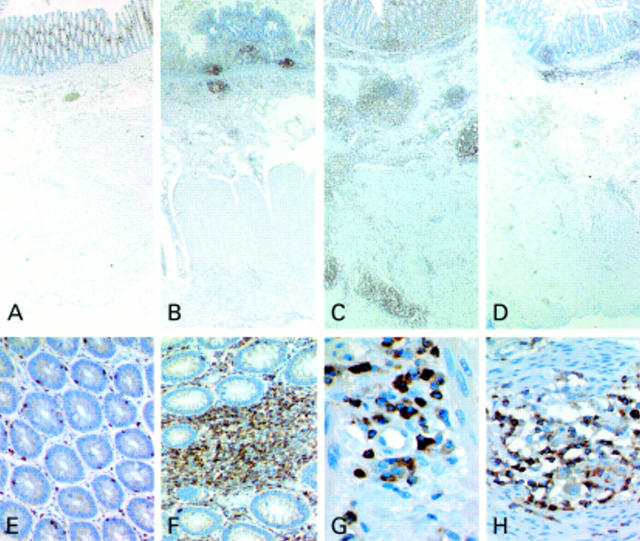
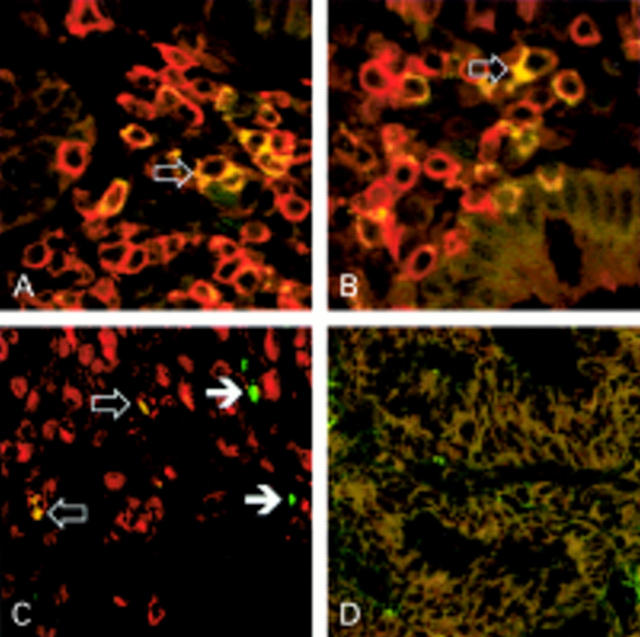
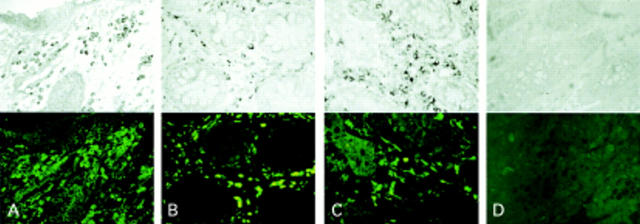
Methods: Expression of IL-16 was analysed in tissue samples of Crohn's disease, ulcerative colitis, and normal controls by applying reverse transcription-polymerase chain reaction, non-radioactive in situ hybridisation, and immunohistochemistry. Double staining methods were used to characterise cells expressing IL-16. The amount of infiltrating CD4+ cells was determined by immunohistochemistry and correlated with the corresponding IL-16+ cell number by step sections.
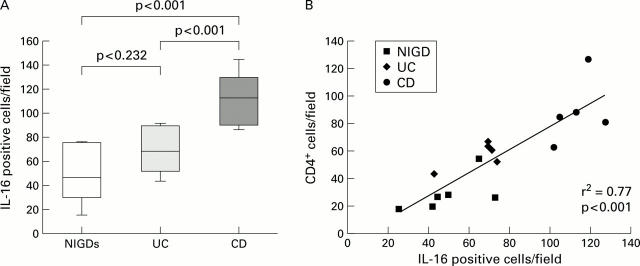
Results: An increased number of IL-16+ cells in Crohn's disease in comparison with ulcerative colitis and control probes was demonstrated. IL-16 was expressed by CD4 and CD8 positive T cells. In addition, in active Crohn's disease there was a substantial number of IL-16 positive mast cells. The increased number of CD4+ lymphocytes correlated positively with the increased number of IL-16 positive cells in Crohn's disease.
Conclusion: Our results demonstrate that increased expression of IL-16 in T cells and mast cells in active Crohn's disease is associated with increased numbers of CD4+ lymphocytes. Local expression of IL-16 seems to play a significant role in the initiation and persistence of the inflammatory process in Crohn's disease, presumably by IL-16 mediated recruitment of CD4+ cells, mostly lymphocytes, into the bowel wall.
Figures
Comment in
-
Monocytes or T cells in Crohn's disease: does IL-16 allow both to play at that game?Gut. 2001 Dec;49(6):747-8. doi: 10.1136/gut.49.6.747. Gut. 2001. PMID: 11709502 Free PMC article. Review. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous