

Review
doi: 10.1136/heart.86.suppl_2.ii3.
Anatomic-echocardiographic correlates: an introduction to normal and congenitally malformed hearts
Affiliations
- PMID: 11709529
- PMCID: PMC1766550
- DOI: 10.1136/heart.86.suppl_2.ii3
Item in Clipboard
Review
Anatomic-echocardiographic correlates: an introduction to normal and congenitally malformed hearts
Heart.
2001 Dec.
No abstract available
Figures
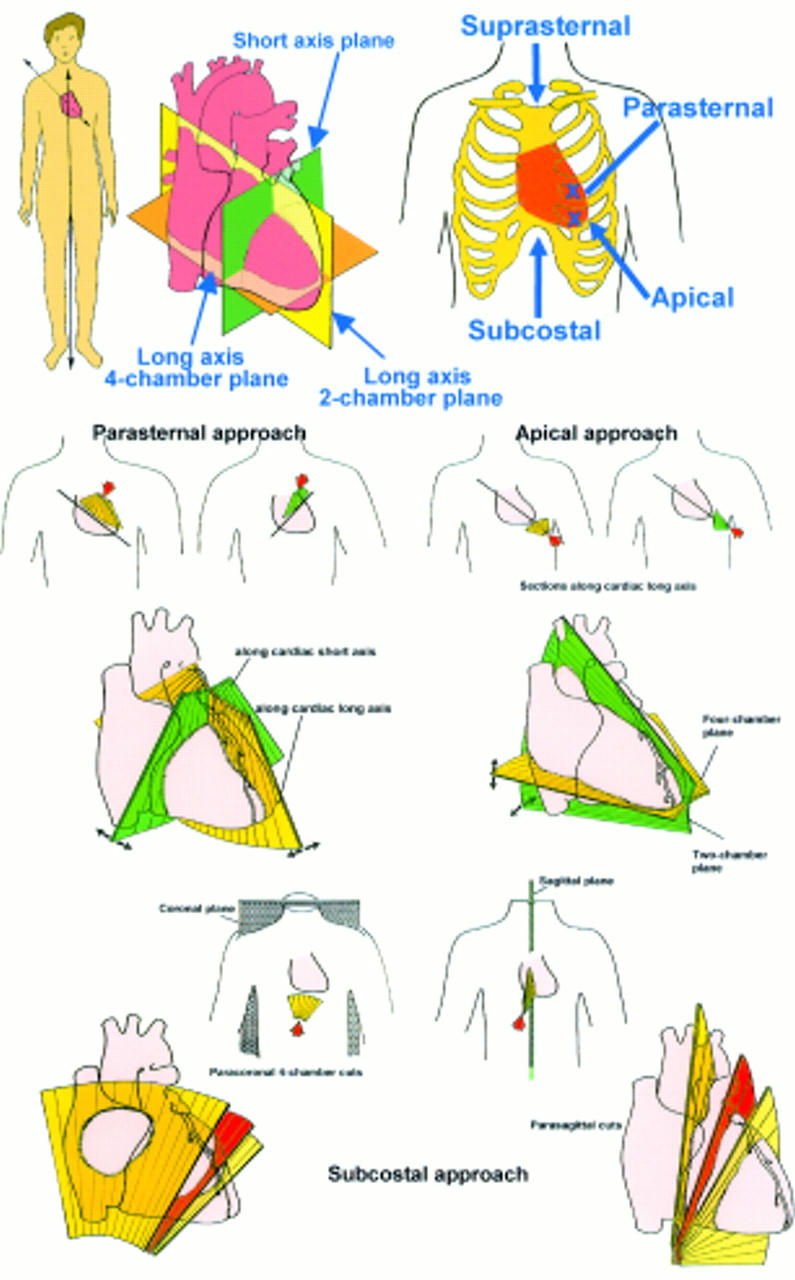
Upper panel: Diagrams showing the orthogonal planes of the body at an angle to that of the heart and the transthoracic windows for accessing the heart. Middle panels: The parasternal approach produces cuts through the short and long axes of the heart itself whereas the apical approach yields long axis two and four chamber cuts. Lower panels: Access from the subcostal window yields short and long axis cuts through the heart that are in parasagittal and paracoronal planes of the body.
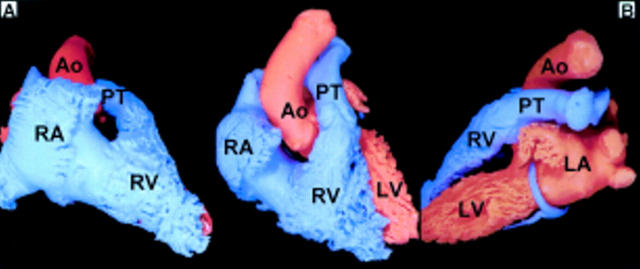
The middle panel shows the endocast viewed from the front displaying mainly the right heart chambers (in blue) and very little of the left heart chambers (in red). When viewed from the right (A), the right heart chambers are to either side of the aorta. The view from the left (B) shows the relation between the right and left ventricular outflow tracts and the posterior location of the left atrium. Ao, aorta; LA, left atrium; LV, left ventricle; RV, right ventricle; PT, pulmonary trunk; RV, right ventricle.
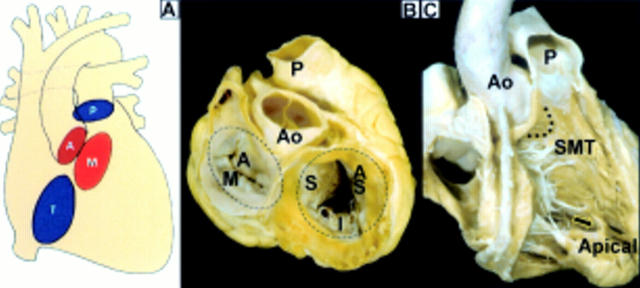
(A) The pulmonary (P), aortic (A), mitral (M), and tricuspid (T) valves are offset from one another. (B) When viewed from the base, the aortic valve(Ao) is centrally located and tucked into the waist of the figure-of-eight arrangement formed by mitral and tricuspid valves. The aortic, or "anterior", leaflet (A) of the mitral valve occupies a shorter circumference than the mural (M) leaflet. The three leaflets of the tricuspid valve are designated septal (S), anterosuperior (AS), and inferior (I). (C)The right heart valves are separated by the ventriculo-infundibular fold (dotted line) which lies between the limbs of the septomarginal trabeculation (SMT). Note the free standing muscular sleeve underneath the pulmonary valve that is the outlet portion of the right ventricle. The inlet portion contains the tricuspid valvar apparatus and the apical portion is coarsely trabeculated. Arrow = moderator band.
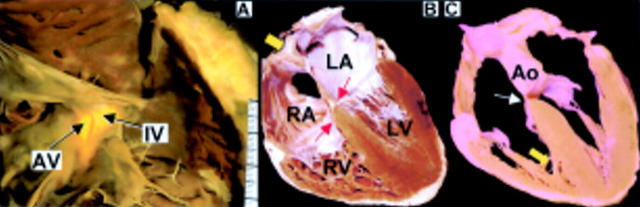
(A) The membranous septum is revealed by transillumination in this view of the right atrium and right ventricle. The hingeline of the tricuspid valve divides the membranous septum into atrioventricular (AV) and interventricular (IV) components. (B)This four chamber section shows the more apical attachment of the tricuspid valve compared to the mitral valve resulting in an offset arrangement (arrows). The cardiac septum is profiled showing the thin valve of the oval fossa. Superiorly, the rim is an infolding of the atrial wall (arrow). (C) A cut taken slightly more cephalad passes through the aortic root producing the so-called five chambers section that shows the aortic valve wedged between the atrioventricular valves. Note the thin membranous septum (small arrow) and the moderator band (thick yellow arrow).
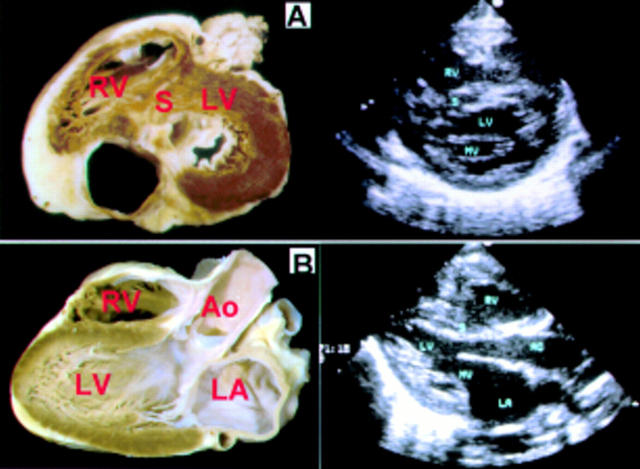
(A) This short axis section shows the mitral valve (MV) in fibrous continuity with the aortic valve. The corresponding echocardiographic section shows the arrangement of the mitral leaflets. (B) This cut shows a long axis section that replicates a parasternal or apical view. Ao, aorta; LA, left atrium; LV, left ventricle; RV, right ventricle; S, septum.
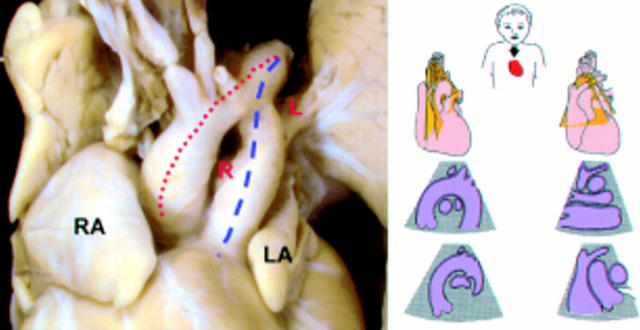
This specimen from a neonate shows the aortic arch giving rise to neck and arm arteries while the pulmonary trunk branches into the right (R) and left (L) pulmonary arteries. The aortic arch (red dotted line) is more superiorly situated than the ductal arch (blue dotted line). Note the distinctive shapes of the right (RA) and left (LA) atrial appendages. The diagram shows cuts that can be obtained from the suprasternal approach.
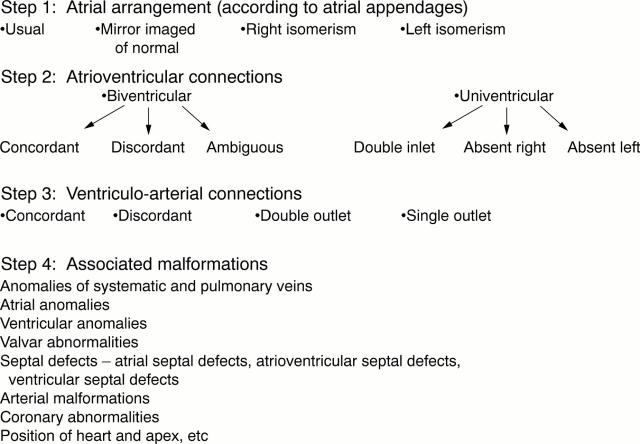
Steps in sequential segmental analysis.
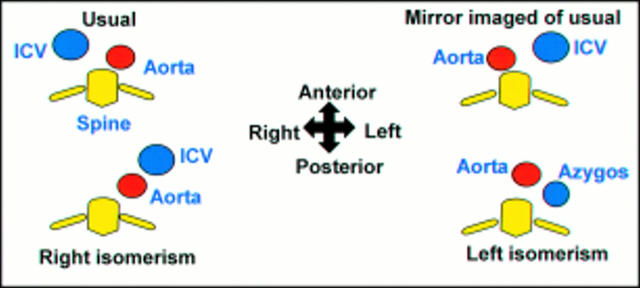
The relative positions of the aorta and the inferior caval vein (ICV) in the subdiaphragmatic region at the level of T11 giving clues to atrial situs.
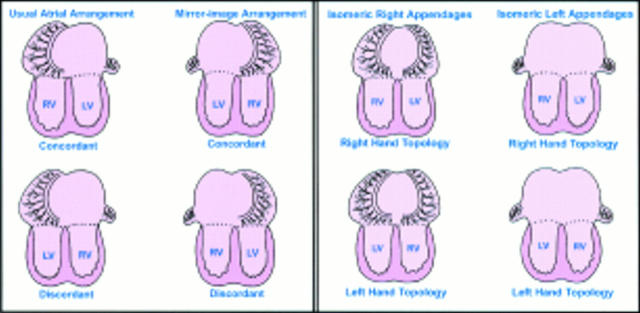
Biventricular atrioventricular connections with lateralised and isomeric arrangements of atrial appendages.

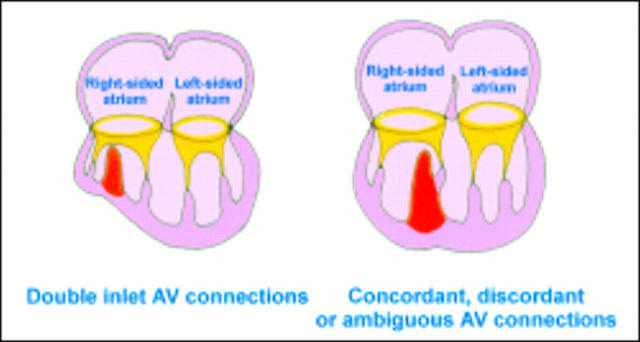
Univentricular atrioventricular connections can exist with any of the four variants of atrial arrangement and any of the three variants of ventricular morphology.
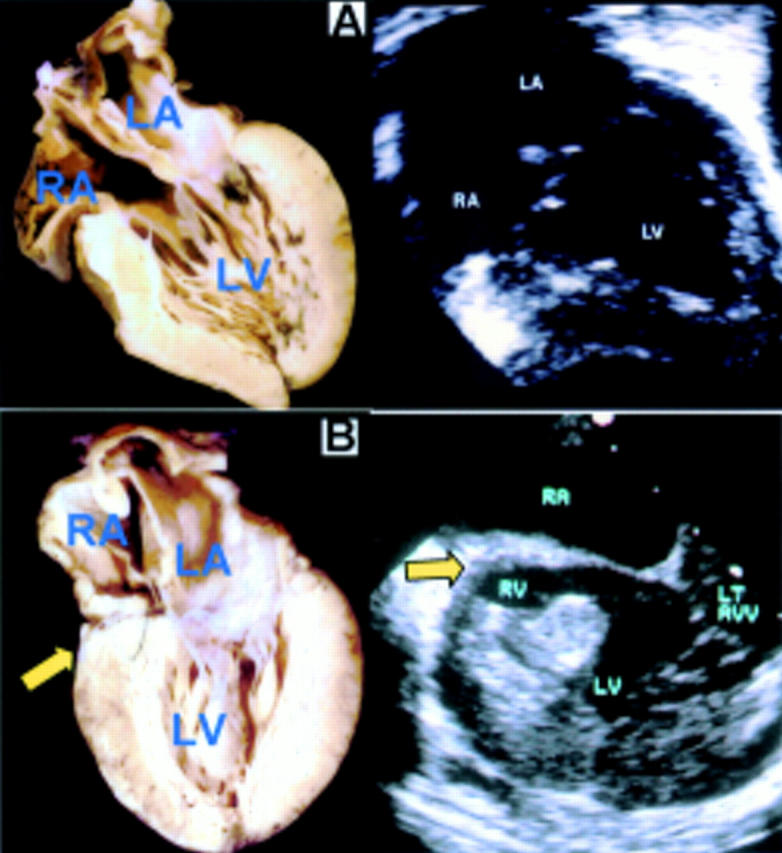
Long axis sections showing (A) double inlet left ventricle and (B) absence of the right atrioventricular connection. The arrow indicates the wedge of fibro-fatty tissue at the atrioventricular groove. LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; LT AVV, left atrioventricular valve.
The 50% rule is used to adjudicate the degree of override distinguishing between univentricular and biventricular atrioventricular connections.
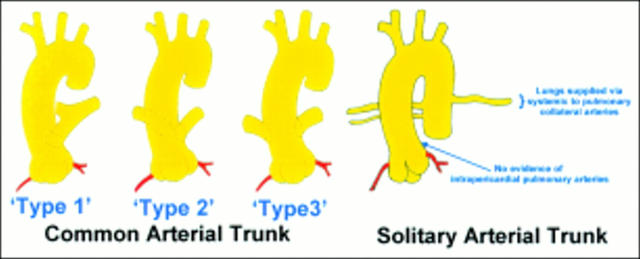
Variants of common arterial trunk compared with the solitary arterial trunk.
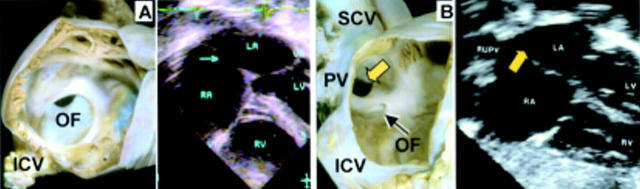
(A) Right atrial view of an oval fossa defect and a similar defect (arrow) seen on four chamber section. (B) Right atrial view shows the superior sinus venosus defect (thick yellow arrow) beneath the orifice of the superior caval vein (SCV) and anomalous insertion of the right pulmonary vein (PV). The oval fossa (OF) is intact. The echocardiographic section shows the defect (arrow) superior to the intact atrial septum and anomalous right upper pulmonary vein (RUPV). ICV, inferior caval vein; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
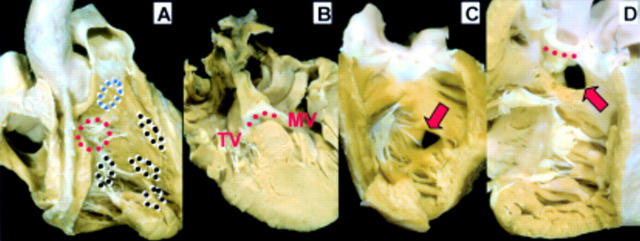
(A) The locations of perimembranous (red circles), muscular (black circles), and doubly committed (blue circles) subtypes of ventricular septal defects are superimposed on this right ventricular view. (B) This four chamber cut through a perimembranous inlet ventricular septal defect shows the fibrous continuity (red dotted line) between tricuspid (TV) and mitral (MV) valves forming the roof of the defect. The normal offset between the valves is lost. (C) The muscular defect (arrow) has complete muscular borders. (D) The doubly committed and juxta-arterial defect (arrow) is roofed by fibrous continuity (red dotted line) between the aortic and pulmonary valves.
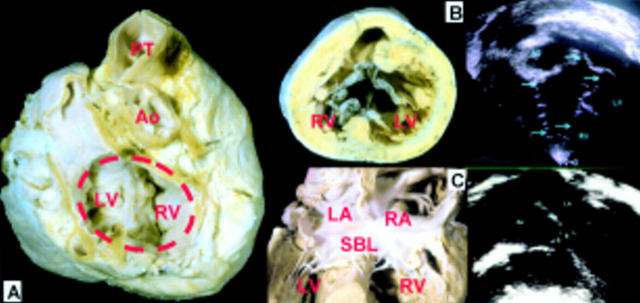
(A) The characteristic feature of a heart with atrioventricular septal defects is the oval shaped common atrioventricular junction (compare with fig 3B) and the anteriorly positioned aorta (Ao) as shown in this case with separate left and right valvar orifices. (B) Short axis cuts through the ventricle viewed from the apex show a common valve with five leaflets. The arrows indicate the peripheral parts between adjacent leaflets. (C) A long axis section of a specimen showing the superior bridging leaflet (SBL) with attachments to both ventricles and a corresponding echocardiographic section. LA, left atrium; LV, left ventricle; PT, pulmonary trunk, RA, right atrium; RV, right ventricle.
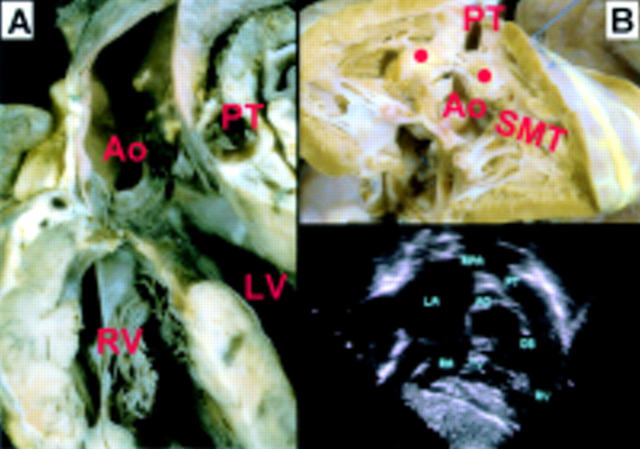
(A) Biventricular connections of the aortic valve (overriding Ao) is shown in this longitudinal section through a heart with tetralogy of Fallot. Note the small calibre of the pulmonary trunk (PT). (B) A specimen displayed in right anterior oblique view with the outlet septum cut through (spots). The insertion of the outlet septum together with hypertrophy of the outlet musculature produces subpulmonary stenosis. The aortic valve is visible through the ventricular septal defect which is cradled between the limbs of the septomarginal trabeculation (SMT). The subcostal cut shows the hallmark of anterocephalad deviation of the outlet septum (OS) narrowing the right ventricular outflow tract in tetralogy of Fallot. LA, left atrium; RA, right atrium; RPA, right pulmonary artery; RV, right ventricle.

The long axis section of a specimen and an echocardiographic section in the same plane show the parallel arrangement of the aorta and pulmonary trunk in cases with complete transposition of the great arteries. Ao, aorta; LA, left atrium; PT, pulmonary trunk; RA, right atrium; RV, right ventricle.
Similar articles
-
Conventional roentgen examination in congenital heart disease.Radiol Clin Biol. 1970;39(2):89-101. Radiol Clin Biol. 1970. PMID: 5426159 No abstract available.
-
[Chest survey films for isolated congenital heart defects in infants and children (author's transl)].Fortschr Geb Rontgenstr Nuklearmed. 1973 Aug;119(2):147-50. Fortschr Geb Rontgenstr Nuklearmed. 1973. PMID: 4357577 German. No abstract available.
-
Axial cineangiography in congenital heart disease.Radiol Clin North Am. 1980 Dec;18(3):515-46. Radiol Clin North Am. 1980. PMID: 7455041
-
Transoesophageal echocardiography in adult congenital heart disease.Heart. 2001 Dec;86 Suppl 2(Suppl 2):II30-II40. doi: 10.1136/heart.86.suppl_2.ii30. Heart. 2001. PMID: 11709532 Free PMC article. Review. No abstract available.
-
The roentgen diagnosis of congenital heart disease.Cardiovasc Clin. 1970;2(1):115-37. Cardiovasc Clin. 1970. PMID: 4255637 Review. No abstract available.
Cited by
-
Association of promoter methylation statuses of congenital heart defect candidate genes with Tetralogy of Fallot.J Transl Med. 2014 Jan 31;12:31. doi: 10.1186/1479-5876-12-31. J Transl Med. 2014. PMID: 24479926 Free PMC article.
-
Anatomy of the atrial septum and interatrial communications.J Thorac Dis. 2018 Sep;10(Suppl 24):S2837-S2847. doi: 10.21037/jtd.2018.02.18. J Thorac Dis. 2018. PMID: 30305943 Free PMC article. Review.
-
Methylation status of CpG sites in the NOTCH4 promoter region regulates NOTCH4 expression in patients with tetralogy of Fallot.Mol Med Rep. 2020 Nov;22(5):4412-4422. doi: 10.3892/mmr.2020.11535. Epub 2020 Sep 24. Mol Med Rep. 2020. PMID: 33000281 Free PMC article.
-
CpG island shore methylation of ZFPM2 is identified in tetralogy of fallot samples.Pediatr Res. 2016 Jul;80(1):151-8. doi: 10.1038/pr.2016.42. Epub 2016 Mar 9. Pediatr Res. 2016. PMID: 26959486
-
De novo 9q gain in an infant with tetralogy of Fallot with absent pulmonary valve: Patient report and review of congenital heart disease in 9q duplication syndrome.Am J Med Genet A. 2015 Dec;167A(12):2966-74. doi: 10.1002/ajmg.a.37296. Epub 2015 Aug 19. Am J Med Genet A. 2015. PMID: 26768185 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical