

Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: a step towards classification as a distinct cardiomyopathy
- PMID: 11711464
- PMCID: PMC1730012
- DOI: 10.1136/heart.86.6.666
Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: a step towards classification as a distinct cardiomyopathy
Abstract
Aim: To determine clear cut echocardiographic criteria for isolated ventricular non-compaction (IVNC), a cardiomyopathy as yet "unclassified" by the World Health Organization. The disease is not widely known and its diagnosis mostly missed.
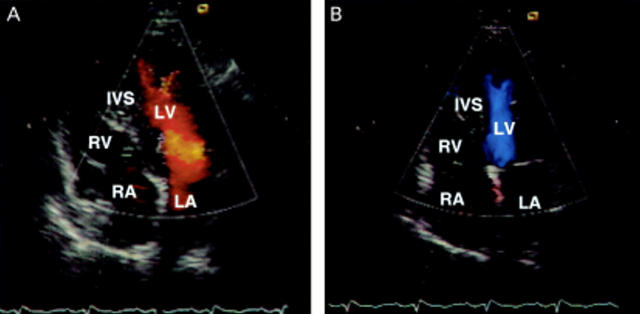
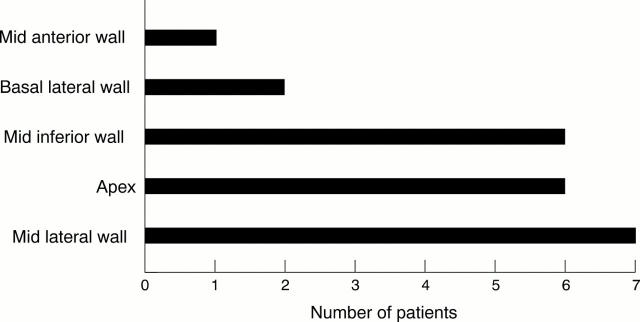
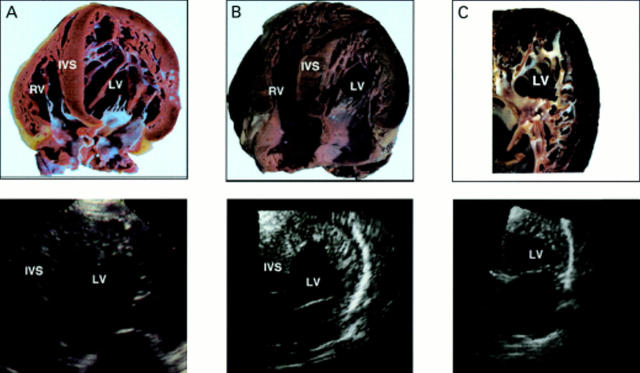
Methods and results: In seven out of a series of 34 patients with IVNC the in vivo echocardiographic characteristics were validated against the anatomical examination of the heart removed after death in four and due to heart transplantation in three patients. Four morphological criteria diagnostic for IVNC were found. (1) Coexisting cardiac abnormalities were absent (by definition). (2) A two layer structure was seen, with a compacted thin epicardial band and a much thicker non-compacted endocardial layer of trabecular meshwork with deep endomyocardial spaces. A maximal end systolic ratio of non-compacted to compacted layers of > 2 is diagnostic. (3) The predominant localisation of the pathology was to mid-lateral (seven of seven patients), apical (six), and mid-inferior (seven) areas. The pathological preparations confirmed the echocardiographic findings. Concomitant regional hypokinesia was not confined to the non-compacted segments. (4) There was colour Doppler evidence of deep perfused intertrabecular recesses.
Conclusions: Four clear cut echocardiographic diagnostic criteria were established. It is suggested that the WHO classification of cardiomyopathies be reconsidered to include IVNC as a distinct cardiomyopathy.
Figures


Comment in
-
Isolated left ventricular non-compaction: a distinct cardiomyopathy?Heart. 2001 Dec;86(6):599-600. doi: 10.1136/heart.86.6.599. Heart. 2001. PMID: 11711443 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical