

Fatiguing inspiratory muscle work causes reflex reduction in resting leg blood flow in humans
- PMID: 11711580
- PMCID: PMC2278925
- DOI: 10.1111/j.1469-7793.2001.0277k.x
Fatiguing inspiratory muscle work causes reflex reduction in resting leg blood flow in humans
Abstract
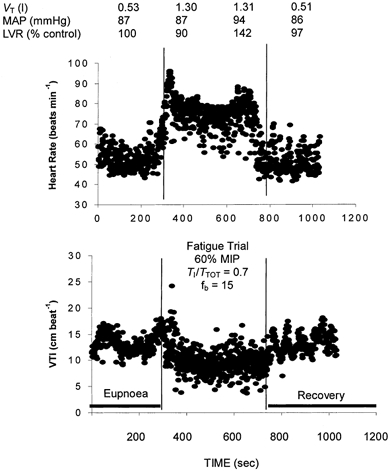
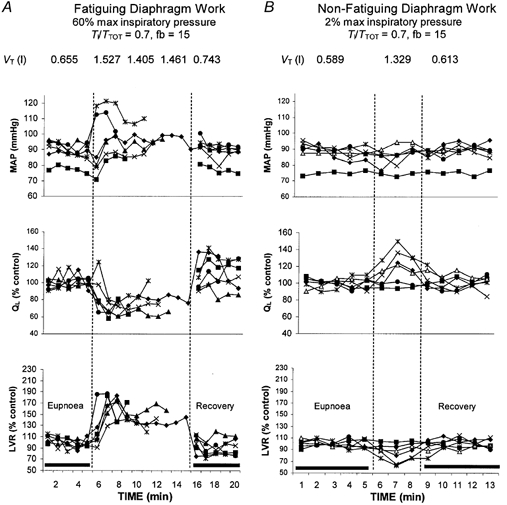
1. We recently showed that fatigue of the inspiratory muscles via voluntary efforts caused a time-dependent increase in limb muscle sympathetic nerve activity (MSNA) (St Croix et al. 2000). We now asked whether limb muscle vasoconstriction and reduction in limb blood flow also accompany inspiratory muscle fatigue. 2. In six healthy human subjects at rest, we measured leg blood flow (.Q(L)) in the femoral artery with Doppler ultrasound techniques and calculated limb vascular resistance (LVR) while subjects performed two types of fatiguing inspiratory work to the point of task failure (3-10 min). Subjects inspired primarily with their diaphragm through a resistor, generating (i) 60 % maximal inspiratory mouth pressure (P(M)) and a prolonged duty cycle (T(I)/T(TOT) = 0.7); and (ii) 60 % maximal P(M) and a T(I)/T(TOT) of 0.4. The first type of exercise caused prolonged ischaemia of the diaphragm during each inspiration. The second type fatigued the diaphragm with briefer periods of ischaemia using a shorter duty cycle and a higher frequency of contraction. End-tidal P(CO2) was maintained by increasing the inspired CO(2) fraction (F(I,CO2)) as needed. Both trials caused a 25-40 % reduction in diaphragm force production in response to bilateral phrenic nerve stimulation. 3. .Q(L) and LVR were unchanged during the first minute of the fatigue trials in most subjects; however, .Q(L) subsequently decreased (-30 %) and LVR increased (50-60 %) relative to control in a time-dependent manner. This effect was present by 2 min in all subjects. During recovery, the observed changes dissipated quickly (< 30 s). Mean arterial pressure (MAP; +4-13 mmHg) and heart rate (+16-20 beats min(-1)) increased during fatiguing diaphragm contractions. 4. When central inspiratory motor output was increased for 2 min without diaphragm fatigue by increasing either inspiratory force output (95 % of maximal inspiratory pressure (MIP)) or inspiratory flow rate (5 x eupnoea), .Q(L), MAP and LVR were unchanged; although continuing the high force output trials for 3 min did cause a relatively small but significant increase in LVR and a reduction in .Q(L). 5. When the breathing pattern of the fatiguing trials was mimicked with no added resistance, LVR was reduced and .Q(L) increased significantly; these changes were attributed to the negative feedback effects on MSNA from augmented tidal volume. 6. Voluntary increases in inspiratory effort, in the absence of diaphragm fatigue, had no effect on .Q(L) and LVR, whereas the two types of diaphragm-fatiguing trials elicited decreases in .Q(L) and increases in LVR. We attribute these changes to a metaboreflex originating in the diaphragm. Diaphragm and forearm muscle fatigue showed very similar time-dependent effects on LVR and .Q(L).
Figures
 , leg blood flow; LVR, limb vascular resistance.
, leg blood flow; LVR, limb vascular resistance.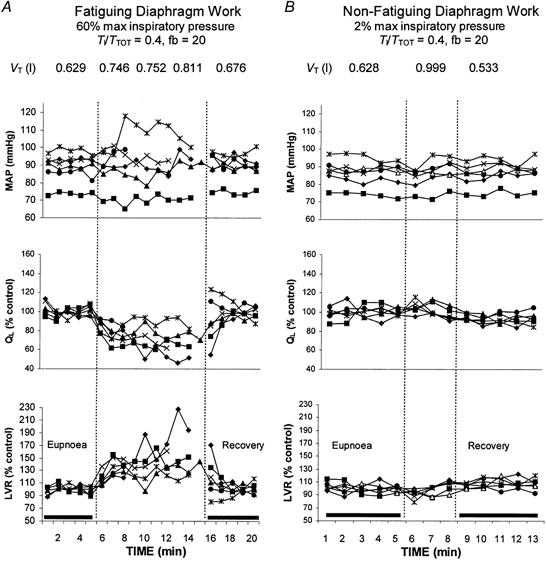 , leg blood flow; LVR, limb vascular resistance.
, leg blood flow; LVR, limb vascular resistance.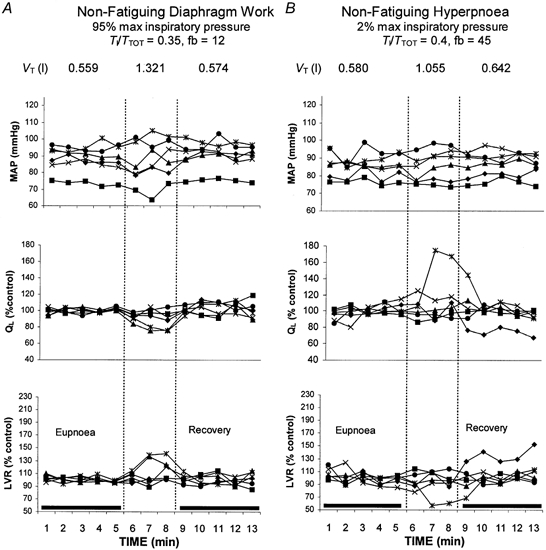 , leg blood flow; LVR, limb vascular resistance.
, leg blood flow; LVR, limb vascular resistance.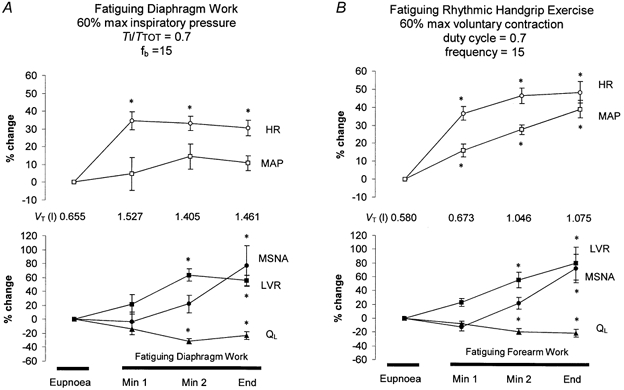 ); ▪, limb vascular resistance (LVR). Values are means ±
); ▪, limb vascular resistance (LVR). Values are means ± Comment in
-
Robin Hood for the lungs? A respiratory metaboreflex that "steals" blood flow from locomotor muscles.J Physiol. 2001 Nov 15;537(Pt 1):2. doi: 10.1111/j.1469-7793.2001.0002k.x. J Physiol. 2001. PMID: 11711555 Free PMC article. No abstract available.
Similar articles
-
Threshold effects of respiratory muscle work on limb vascular resistance.Am J Physiol Heart Circ Physiol. 2002 May;282(5):H1732-8. doi: 10.1152/ajpheart.00798.2001. Am J Physiol Heart Circ Physiol. 2002. PMID: 11959638 Clinical Trial.
-
Effect of increased inspiratory muscle work on blood flow to inactive and active limbs during submaximal dynamic exercise.Exp Physiol. 2019 Feb;104(2):180-188. doi: 10.1113/EP087380. Epub 2018 Dec 9. Exp Physiol. 2019. PMID: 30462876
-
Fatiguing inspiratory muscle work causes reflex sympathetic activation in humans.J Physiol. 2000 Dec 1;529 Pt 2(Pt 2):493-504. doi: 10.1111/j.1469-7793.2000.00493.x. J Physiol. 2000. PMID: 11101657 Free PMC article.
-
Exercise-induced respiratory muscle fatigue: implications for performance.J Appl Physiol (1985). 2008 Mar;104(3):879-88. doi: 10.1152/japplphysiol.01157.2007. Epub 2007 Dec 20. J Appl Physiol (1985). 2008. PMID: 18096752 Review.
-
Monitoring respiratory muscles.Monaldi Arch Chest Dis. 1998 Dec;53(6):640-3. Monaldi Arch Chest Dis. 1998. PMID: 10063336 Review.
Cited by
-
Correlation between handgrip strength and air trapping in patients with stable chronic obstructive pulmonary disease.J Thorac Dis. 2024 Sep 30;16(9):5634-5642. doi: 10.21037/jtd-24-631. Epub 2024 Aug 30. J Thorac Dis. 2024. PMID: 39444886 Free PMC article.
-
A short course of high-resistance, low-volume breathing exercise extends respiratory endurance and blunts cardiovascular responsiveness to constant load respiratory testing in healthy young adults.Respir Physiol Neurobiol. 2023 Jan;307:103974. doi: 10.1016/j.resp.2022.103974. Epub 2022 Sep 27. Respir Physiol Neurobiol. 2023. PMID: 36180018 Free PMC article.
-
Breathing a low-density gas reduces respiratory muscle force development and marginally improves exercise performance in master athletes.Eur J Appl Physiol. 2024 Feb;124(2):651-665. doi: 10.1007/s00421-023-05346-6. Epub 2023 Nov 17. Eur J Appl Physiol. 2024. PMID: 37973652
-
The impact of thoracic load carriage up to 45 kg on the cardiopulmonary response to exercise.Eur J Appl Physiol. 2016 Sep;116(9):1725-34. doi: 10.1007/s00421-016-3427-6. Epub 2016 Jul 9. Eur J Appl Physiol. 2016. PMID: 27395054 Clinical Trial.
-
Does impaired O2 delivery during exercise accentuate central and peripheral fatigue in patients with coexistent COPD-CHF?Front Physiol. 2015 Jan 7;5:514. doi: 10.3389/fphys.2014.00514. eCollection 2014. Front Physiol. 2015. PMID: 25610401 Free PMC article.
References
-
- Babcock MA, Pegelow DF, Johnson BD, Dempsey JA. Aerobic fitness effects on exercise-induced low-frequency diaphragm fatigue. Journal of Applied Physiology. 1996;81:2156–2164. - PubMed
-
- Bellemare F, Wight D, Lavigne CM, Grassino A. Effect of tension and timing of contraction on the blood flow of the diaphragm. Journal of Applied Physiology. 1983;54:1597–1606. - PubMed
-
- Buchler B, Magder S, Kastardis H, Jammes Y, Roussos C. Effects of pleural pressure and abdominal pressure on diaphragmatic blood flow. Journal of Applied Physiology. 1985;58:691–697. - PubMed
-
- Derchak PA, Sheel AW, Morgan BJ, Pegelow DF, Dempsey JA. Effects of expiratory muscle work on muscle sympathetic nerve activity. Journal of Applied Physiology. 2001 (in the Press) - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous