

Factors contributing to anemia after uncomplicated falciparum malaria
- PMID: 11716124
- PMCID: PMC4337986
- DOI: 10.4269/ajtmh.2001.65.614
Factors contributing to anemia after uncomplicated falciparum malaria
Abstract
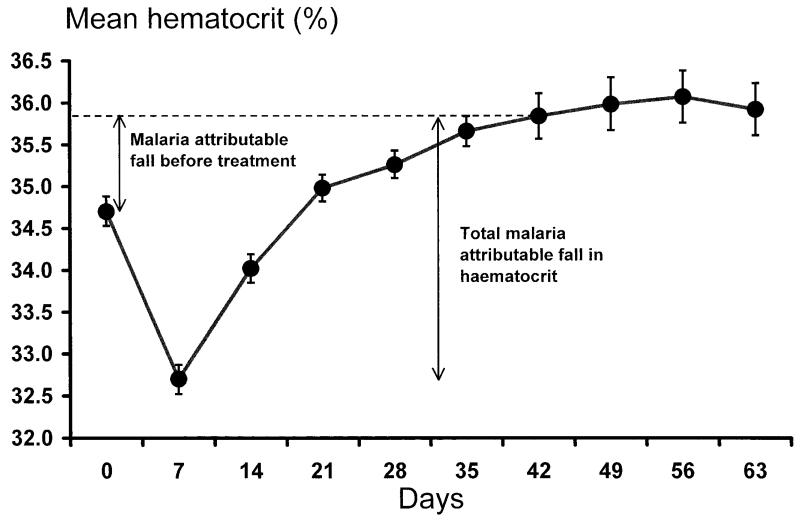
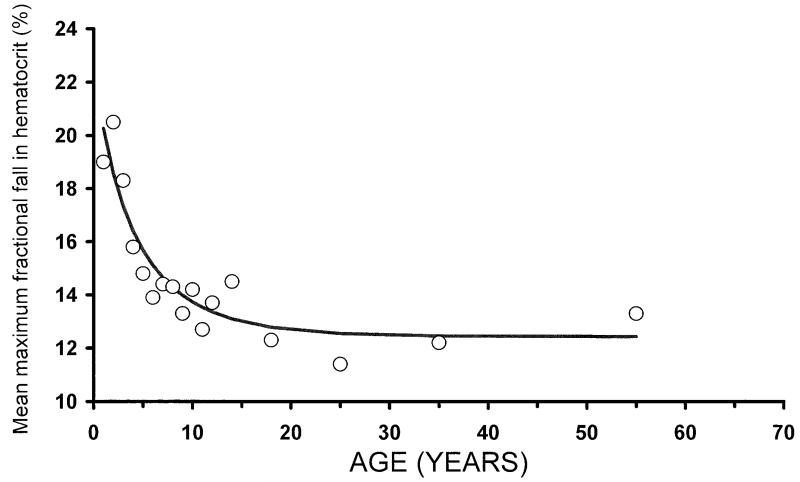
The factors contributing to anemia in falciparum malaria were characterized in 4,007 prospectively studied patients on the western border of Thailand. Of these, 727 patients (18%) presented with anemia (haematocrit < 30%), and 1% (55 of 5,253) required blood transfusion. The following were found to be independent risk factors for anemia at admission: age < 5 years, a palpable spleen, a palpable liver, recrudescent infections, being female, a prolonged history of illness (> 2 days) before admission, and pure Plasmodium falciparum infections rather than mixed P. falciparum and Plasmodium vivax infections. The mean maximum fractional fall in hematocrit after antimalarial treatment was 14.1% of the baseline value (95% confidence interval [CI], 13.6-14.6). This reduction was significantly greater in young children (aged < 5 years) and in patients with a prolonged illness, high parasitemia, or delayed parasite clearance. Loss of parasitized erythrocytes accounted for < 10% of overall red blood cell loss. Hematological recovery was usually complete within 6 weeks, but it was slower in patients who were anemic at admission (adjusted hazards ratio [AHR], 1.9, 95% CI, 1.5-2.3), and those whose infections recrudesced (AHR, 1.2, 95% CI, 1.01-1.5). Half the patients with treatment failure were anemic at 6 weeks compared with 19% of successfully treated patients (relative risk, 2.8, 95% CI, 2.0-3.8). Patients coinfected with P. vivax (16% of the total) were 1.8 (95% CI, 1.2-2.6) times less likely to become anemic and recovered 1.3 (95% CI, 1.0-1.5) times faster than those with P. falciparum only. Anemia is related to drug resistance and treatment failure in uncomplicated malaria. Children aged < 5 years of age were more likely than older children or adults to become anemic. Coinfection with P. vivax attenuates the anemia of falciparum malaria, presumably by modifying the severity of the infection.
Figures

References
-
- Hedberg K, Shaffer N, Davachi F, Hightower A, Lyamba B, Paluku KM, Nguyen Dinh P, Breman JG. Plasmodium falciparum-associated anemia in children at a large urban hospital in Zaire. Am J Trop Med Hyg. 1993;48:365–371. - PubMed
-
- White NJ, Ho M. The pathophysiology of malaria. In: Baker JR, Muller R, editors. Advances in Parasitology. Academic Press; New York: 1992. pp. 84–175. - PubMed
-
- Slutsker L, Taylor TE, Wirima JJ, Steketee RW. In-hospital morbidity and mortality due to malaria-associated severe anaemia in two areas of Malawi with different patterns of malaria infection. Trans R Soc Trop Med Hyg. 1994;88:548–551. - PubMed
-
- Ekvall H, Premji Z, Bjorkman A. Chloroquine treatment for uncomplicated childhood malaria in an area with drug resistance: early treatment failure aggravates anaemia. Trans R Soc Trop Med Hyg. 1998;92:556–560. - PubMed
-
- Bloland PB, Lackritz EM, Kazembe PN, Were JB, Steketee R, Campbell CC. Beyond chloroquine: implications of drug resistance for evaluating malaria therapy efficacy and treatment policy in Africa. J Infect Dis. 1993;167:932–937. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
