

Which treatment for low back pain? A factorial randomised controlled trial comparing intravenous analgesics with oral analgesics in the emergency department and a centrally acting muscle relaxant with placebo over three days [ISRCTN09719705]
- PMID: 11716789
- PMCID: PMC59893
- DOI: 10.1186/1471-227x-1-2
Which treatment for low back pain? A factorial randomised controlled trial comparing intravenous analgesics with oral analgesics in the emergency department and a centrally acting muscle relaxant with placebo over three days [ISRCTN09719705]
Abstract
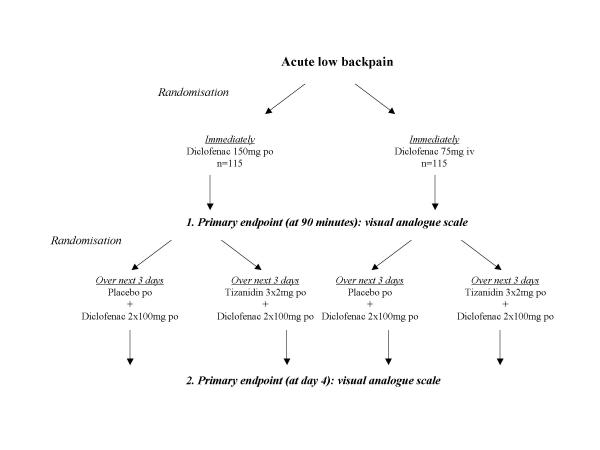
BACKGROUND: About two thirds of adults suffer from backpain at some time during their life. In the emergency room many patients with acute back pain are treated with intravenous non-steroidal analgesics. Whether this treatment is superior to oral administration of non-steroidal analgesics is unknown. Intravenous administration, however, requires considerable amounts of resources and accounts for high workload in busy clinics. In the further course centrally acting muscle relaxants are prescribed but the effectiveness remains unclear. The objective of this study is on the one hand to compare the effectiveness of intravenous with oral non-steroidal analgesics for acute treatment and on the other hand to compare the effectiveness of a centrally active muscle relaxant with placebo given for three days after presentation to the ED (emergency department). METHODS/DESIGN: This study is intended as a randomised controlled factorial trial mainly for two reasons: (1) the sequence of treatments resembles the actual proceedings in every-day clinical practice, which is important for the generalisability of the results and (2) this design allows to take interactions between the two sequential treatment strategies into account. There is a patient preference arm included because patients preference is an important issue providing valuable information: (1) it allows to assess the interaction between desired treatment and outcome, (2) results can be extrapolated to a wider group while (3) conserving the advantages of a fully randomised controlled trial. CONCLUSION: We hope to shed more light on the effectiveness of treatment modalities available for acute low back pain.
Figures
References
-
- Statistisches Zentralamt Gesundheitsbericht der Stadt Wien 2000. [Health report of Vienna 2000] Vienna. 2000.
-
- van Tulder MW, Scholten RJPM, Koes BW, Deyo RA. Non steroidal anti-inflammatory drugs for low back pain (Cochrane Rev) The Cochrane Library. 2000. - PubMed
-
- Bur A, Müllner M, Sterz F, Hirschl MM, Laggner AN. The emergency department in a 2000-bed teaching hospital: saving open ward and intensive care facilities. European Journal of Emergency Medicine. 1997;4:19–33. - PubMed
LinkOut - more resources
Full Text Sources
