

Guillain Barré syndrome
Abstract
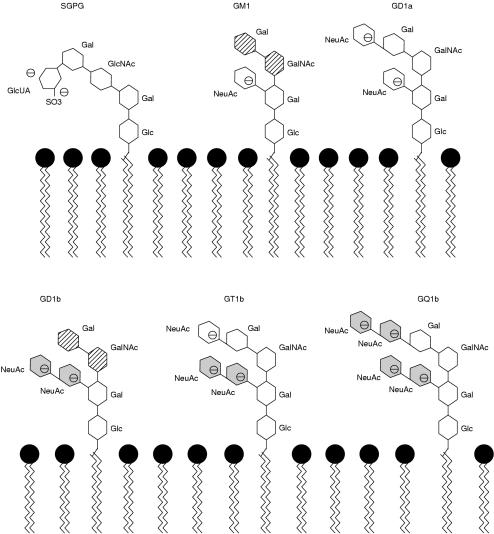
Guillain Barré syndrome is one of the best examples of a post infectious immune disease and offers insights into the mechanism of tissue damage in other more common autoimmune diseases. Controlled epidemiological studies have linked it to infection with Campylobacter jejuni in addition to other viruses including cytomegalovirus and Epstein Barr virus. The syndrome includes several pathological subtypes, of which the most common is a multifocal demyelinating disorder of the peripheral nerves in close association with macrophages. Evidence from histological examination of peripheral nerve biopsy and postmortem samples suggests that both cell mediated and humoral mechanisms are involved in the pathogenesis. Immunological studies suggest that at least one third of patients have antibodies against nerve gangliosides, which in some cases also react with constituents of the liposaccharide of C jejuni. In the Miller Fisher variant of the disease, these antiganglioside antibodies have been shown to produce neuromuscular block, and may in part explain the clinical signs of that disorder. Treatment with both intravenous immunoglobulin and plasma exchange reduces the time taken for recovery to occur, although mortality remains around 8%, with about 20% of patients remaining disabled.
Figures
Similar articles
-
New concepts of Guillain-Barré syndrome.J Child Neurol. 2000 Mar;15(3):183-91. doi: 10.1177/088307380001500308. J Child Neurol. 2000. PMID: 10757475 Review.
-
Guillain-Barré syndrome.Lancet. 2005 Nov 5;366(9497):1653-66. doi: 10.1016/S0140-6736(05)67665-9. Lancet. 2005. PMID: 16271648 Review.
-
Does Campylobacter jejuni infection elicit "demyelinating" Guillain-Barre syndrome?Neurology. 2004 Aug 10;63(3):529-33. doi: 10.1212/01.wnl.0000133205.05169.04. Neurology. 2004. PMID: 15304587
-
Guillain Barré Syndrome is induced in Non-Obese Diabetic (NOD) mice following Campylobacter jejuni infection and is exacerbated by antibiotics.J Autoimmun. 2017 Feb;77:11-38. doi: 10.1016/j.jaut.2016.09.003. Epub 2016 Dec 9. J Autoimmun. 2017. PMID: 27939129
-
Guillain-Barré syndrome.Lancet. 2016 Aug 13;388(10045):717-27. doi: 10.1016/S0140-6736(16)00339-1. Epub 2016 Mar 2. Lancet. 2016. PMID: 26948435 Review.
Cited by
-
An unusual case of Parinaud's syndrome.BMJ Case Rep. 2012 Nov 21;2012:bcr2012006722. doi: 10.1136/bcr-2012-006722. BMJ Case Rep. 2012. PMID: 23175005 Free PMC article.
-
Guillain-Barré syndrome in a Child with Ongoing Viral Hepatitis A.Iran J Child Neurol. 2018 Summer;12(3):133-138. Iran J Child Neurol. 2018. PMID: 30026778 Free PMC article.
-
Epidemiology of Guillain-Barré Syndrome in Iranian Children Aged 0-15 Years (2008-2013).Iran J Child Neurol. 2021 Fall;15(4):27-34. doi: 10.22037/ijcn.v15i4.25087. Iran J Child Neurol. 2021. PMID: 34782839 Free PMC article.
-
The Pathogenic Role of Ganglioside Metabolism in Alzheimer's Disease-Cholinergic Neuron-Specific Gangliosides and Neurogenesis.Mol Neurobiol. 2017 Jan;54(1):623-638. doi: 10.1007/s12035-015-9641-0. Mol Neurobiol. 2017. PMID: 26748510 Review.
-
Role of Campylobacter jejuni infection in the pathogenesis of Guillain-Barré syndrome: an update.Biomed Res Int. 2013;2013:852195. doi: 10.1155/2013/852195. Epub 2013 Aug 13. Biomed Res Int. 2013. PMID: 24000328 Free PMC article. Review.
References
-
- Guillain G, Barré J, Strohl A. Sur un syndrome de radiculo-nevrite avec hyperalbuminose du liquide cephalorachidien sans reaction cellulaire. Remarques sur les characteres clinique et graphique des reflexes tendinaux. Bulletins et Memories de la Societe Medicale des Hopitaux de Paris 1916;40:1462–70.
-
- Alter M. The epidemiology of Guillain-Barré syndrome. Ann Neurol 1990:27(suppl):S7–12. - PubMed
-
- Kaplan JE, Katona P, Hurwitz ES, et al. Guillain-Barré syndrome in the United States, 1979–1980 and 1980–1981. Lack of an association with influenza vaccination. JAMA 1982;248:698–700. - PubMed
-
- Carpo M, Pedotti R, Allaria S, et al. Clinical presentation and outcome of Guillain-Barré and related syndromes in relation to anti-ganglioside antibodies. J Neurol Sci 1999;168:78–84. - PubMed
-
- Yuki N. Molecular mimicry between gangliosides and lipopolysaccharides of Campylobacter jejuni isolated from patients with Guillain-Barré syndrome and Miller Fisher syndrome. J Infect Dis 1997;176(suppl 2):S150–3. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical