

Influence of resection margins on survival for patients with pancreatic cancer treated by adjuvant chemoradiation and/or chemotherapy in the ESPAC-1 randomized controlled trial
- PMID: 11729382
- PMCID: PMC1422135
- DOI: 10.1097/00000658-200112000-00007
Influence of resection margins on survival for patients with pancreatic cancer treated by adjuvant chemoradiation and/or chemotherapy in the ESPAC-1 randomized controlled trial
Abstract
Objective: To assess the influence of resection margins on survival for patients with resected pancreatic cancer treated within the context of the adjuvant European Study Group for Pancreatic Cancer-1 (ESPAC-1) study.
Summary background data: Pancreatic cancer is associated with a poor long-term survival rate of only 10% to 15% after resection. Patients with positive microscopic resection margins (R1) have a worse survival, but it is not known how they fare in adjuvant studies.
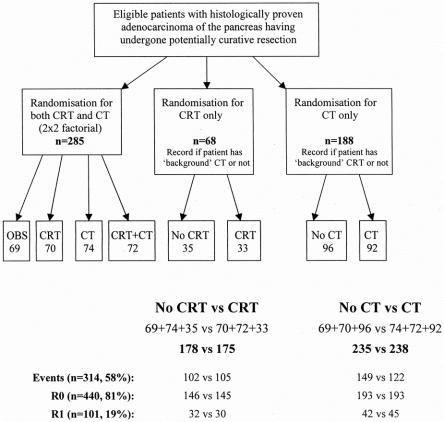
Methods: ESPAC-1, the largest randomized adjuvant study of resectable pancreatic cancer ever performed, set out to look at the roles of chemoradiation and chemotherapy. Randomization was stratified prospectively by resection margin status.
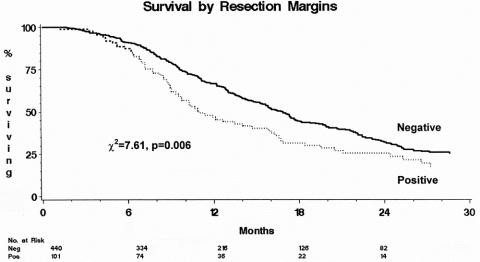
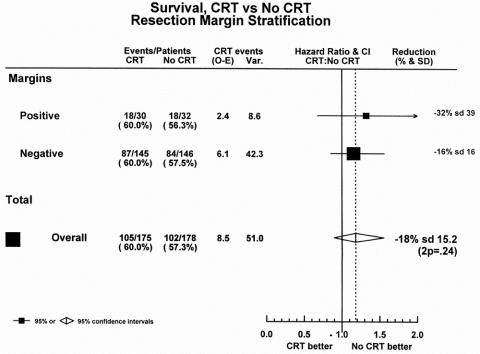
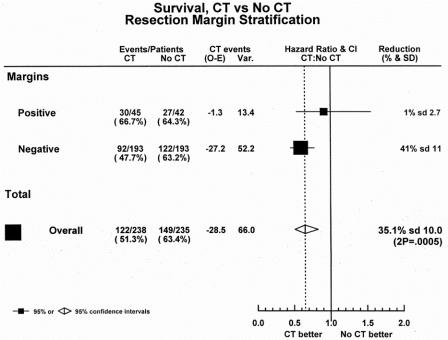
Results: Of 541 patients with a median follow-up of 10 months, 101 (19%) had R1 resections. Resection margin status was confirmed as an influential prognostic factor, with a median survival of 10.9 months for R1 versus 16.9 months months for patients with R0 margins. Resection margin status remained an independent factor in a Cox proportional hazards model only in the absence of tumor grade and nodal status. There was a survival benefit for chemotherapy but not chemoradiation, irrespective of R0/R1 status. The median survival was 19.7 months with chemotherapy versus 14.0 months without. For patients with R0 margins, chemotherapy produced longer survival compared with to no chemotherapy. This difference was less apparent for the smaller subgroup of R1 patients, but there was no significant heterogeneity between the R0 and R1 groups.
Conclusions: Resection margin-positive pancreatic tumors represent a biologically more aggressive cancer; these patients benefit from resection and adjuvant chemotherapy but not chemoradiation. The magnitude of benefit for chemotherapy treatment is reduced for patients with R1 margins versus those with R0 margins. Patients with R1 tumors should be included in future trials of adjuvant treatments and randomization and analysis should be stratified by this significant prognostic factor.
Figures
Comment in
-
ESPAC-1 trial of adjuvant therapy for resectable adenocarcinoma of the pancreas.Ann Surg. 2002 Nov;236(5):694; author reply 694-6. doi: 10.1097/01.SLA.0000037256.09376.FC. Ann Surg. 2002. PMID: 12409677 Free PMC article. No abstract available.
References
-
- Parkin DM, Muir CS, Whelan SL, et al. Cancer incidence in five continents. Vol. VI. Lyon: International Agency for Research on Cancer, 1992 (IARC Scientific Publications No. 120) Oxford University Press.
-
- Bramhall SR, Allum WH, Jones AG, et al. Incidence, treatment and survival in 13,560 patients with pancreatic cancer: an epidemiological study in the West Midlands. Br J Surg 1995; 82: 111–115. - PubMed
-
- Boring CC, Squires TS, Tong T, et al. Cancer statistics. CA Cancer J Clin 1994; 44: 7–26. - PubMed
-
- Neoptolemos JP, Russell RCG, Bramhall SR, et al. Low mortality following resection for pancreatic and periampullary tumors in 1026 patients: UK survey of specialist pancreatic units. Br J Surg 1997; 84: 1370–1376. - PubMed
-
- Begg CB, Cramer LD, Hoskins WJ, et al. Impact of hospital volume on operative mortality for major cancer surgery. JAMA 1998; 280: 1747–1751. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
