

A new surgical concept for rectal replacement after low anterior resection: the transverse coloplasty pouch
- PMID: 11729384
- PMCID: PMC1422137
- DOI: 10.1097/00000658-200112000-00009
A new surgical concept for rectal replacement after low anterior resection: the transverse coloplasty pouch
Abstract
Objective: To analyze the feasibility, safety, complication and death rates, and early functional results of the transverse coloplasty pouch procedure after low anterior rectal resection and total mesorectal excision.
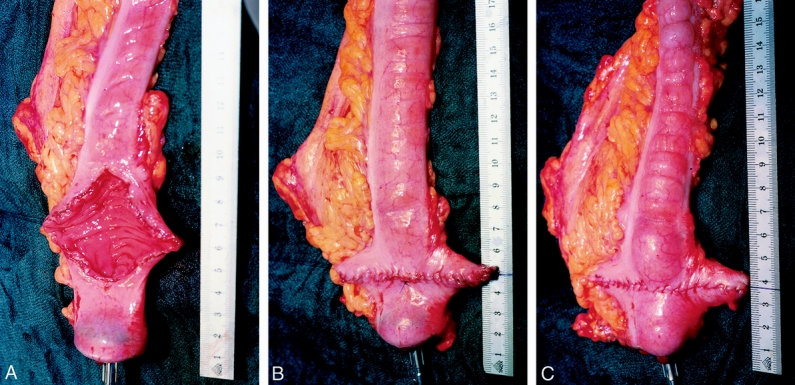
Summary background data: The authors previously developed a novel neorectal reservoir, the transverse coloplasty pouch, in an animal model; they report the first clinical data of a prospective phase 1 study.
Methods: Forty-one patients underwent low anterior rectal resection with total mesorectal excision for rectal cancer (n = 37) or benign pathology (n = 4). The continuity was restored with a transverse coloplasty pouch anastomosis, and the colon was defunctionalized for 3 months. Patients were followed up at 2-month intervals for functional outcome.
Results: Intraoperative complications occurred in three patients (7%), none related to the transverse coloplasty pouch. There were no hospital deaths and the total complication rate was 27% (11/41); an anastomotic leakage rate of 7% was recorded. The stool frequency was 3.4 per 24 hours at 2 months follow-up and gradually decreased to 2.1 per 24 hours at 8 months. Stool dysfunctions such as stool urgency, fragmentation, and incontinence grade 1 and 2 were regularly observed until 6 months; the incidence significantly decreased thereafter. None of the patients had difficulties in pouch evacuation.
Conclusions: The transverse coloplasty pouch is a small-volume reservoir that can safely be used for reconstruction after sphincter-preserving rectal resection. The early functional outcome is favorable and can be compared to other colonic reservoirs. The concept of reducing early dysfunction seen after straight coloanal anastomosis and avoiding long-term problems of pouch evacuation is supported by this study. Future trials will compare the transverse coloplasty pouch with other techniques of restorative resections of the rectum.
Figures
References
-
- Lazorthes F, Fages P, Chiotasso P, et al. Resection of the rectum with construction of a colonic reservoir and colo-anal anastomosis for carcinoma of the rectum. Br J Surg 1986; 73: 136–138. - PubMed
-
- Parc R, Tiret E, Frileux P, et al. Resection and colo-anal anastomosis with colonic reservoir for rectal carcinoma. Br J Surg 1986; 73: 139–141. - PubMed
-
- Ho YH, Tan M, Seow-Choen F. Prospective randomized controlled study of clinical function and anorectal physiology after low anterior resection: comparison of straight and colonic J pouch anastomoses. Br J Surg 1996; 83: 978–980. - PubMed
-
- Seow-Choen F, Goh HS. Prospective randomized trial comparing J colonic pouch-anal anastomosis and straight coloanal reconstruction. Br J Surg 1995; 82: 608–610. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
