

Aneurysmal rupture during embolization with Guglielmi detachable coils: causes, management, and outcome
- PMID: 11733309
- PMCID: PMC7973837
Aneurysmal rupture during embolization with Guglielmi detachable coils: causes, management, and outcome
Abstract
Background and purpose: Aneurysmal rupture during endovascular treatment is one of the most feared complications of endovascular aneurysm therapy. The purpose of this study was to determine the frequency, causes, management, and outcome of aneurysmal rupture that occurred during treatment with Guglielmi detachable coils (GDCs) in an unselected series of patients with ruptured cerebral aneurysms.
Methods: Between July 1997 and December 2000, we treated 164 acutely ruptured cerebral aneurysms with GDCs. All charts were reviewed, and patients with aneurysmal rupture occurring during embolization were identified.
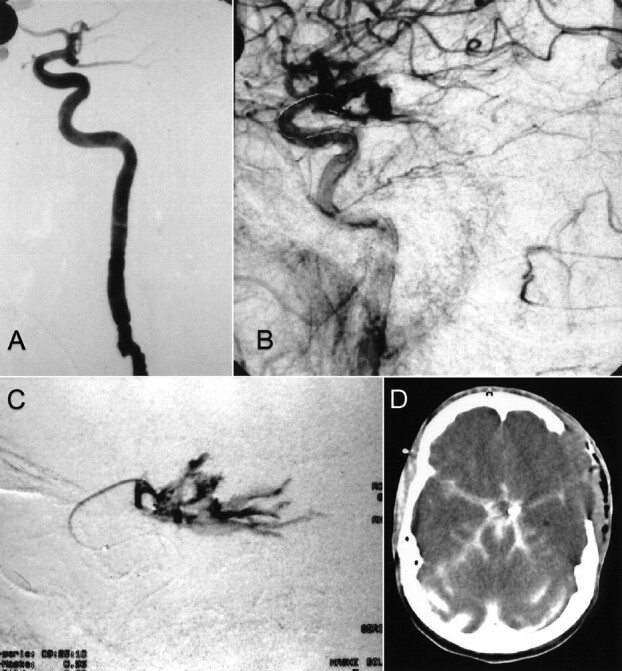
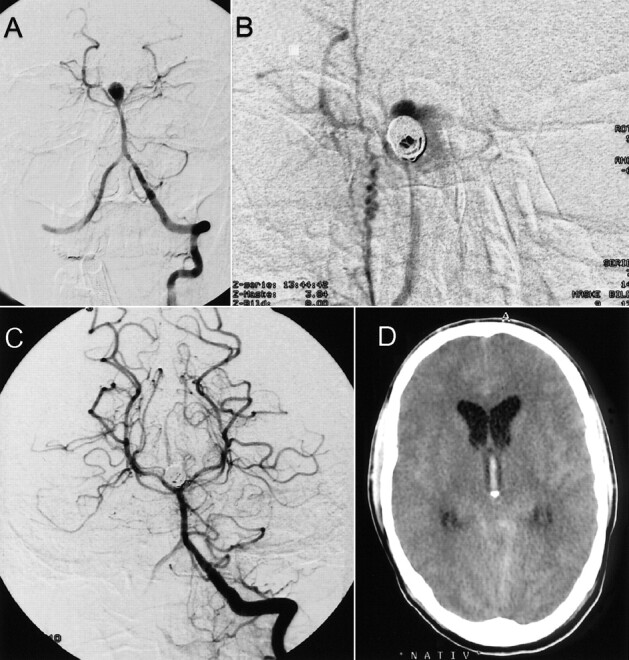
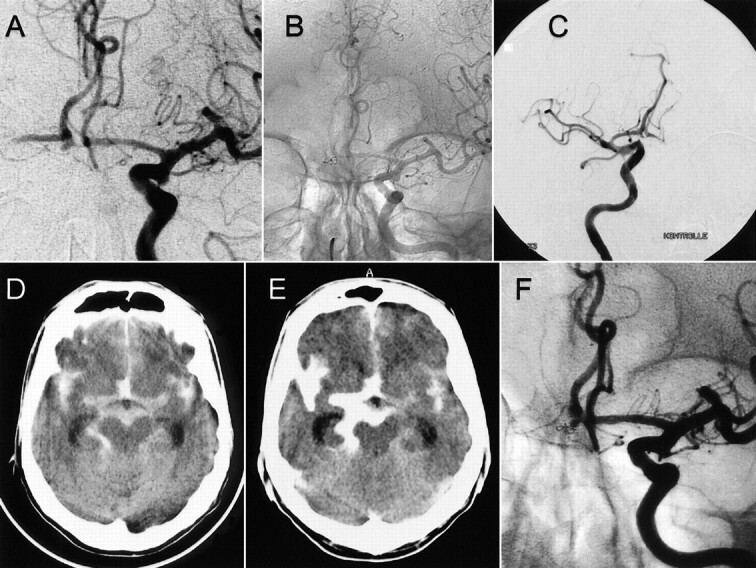
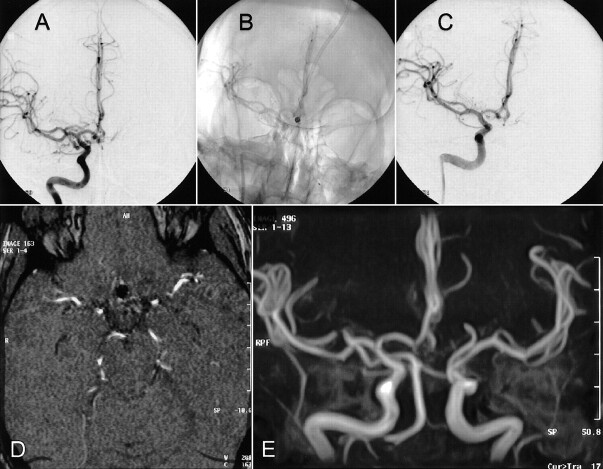
Results: Five patients had an intraprocedural aneurysmal rupture. In one patient, rupture was due to guidewire perforation of the wall. In two patients, the microcatheter itself perforated the aneurysm. In another two patients, rupture occurred during placement of the first coil. Endovascular packing was continued in all patients. One patient died as a result of the aneurysmal rupture. No negative long-term effects were observed in the remaining four patients. In summary, we observed intraprocedural aneurysmal rupture in 3% of our patients, with a mortality rate of 20% and no long-term morbidity.
Conclusion: Aneurysmal rupture during endovascular treatment with GDCs is a rare event; clinical severity may be variable. Embolization of the aneurysm can be continued in most cases, and most patients with treatment-related subarachnoid hemorrhage survive without serious sequelae.
Figures
References
-
- Serbinenko FA. Balloon catheterization and occlusion of major cerebral vessels. J Neurosurg 1974;41:125-145 - PubMed
-
- Guglielmi G, Viñuela F, Sepetka I, Macellari V. Electrothrombosis of saccular aneurysms via endovascular approach, I: electrochemical basis, technique, and experimental results. J Neurosurg 1991;75:1-7 - PubMed
-
- Viñuela F, Duckwiler G, Mawad M. Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 1997;86:475-482 - PubMed
-
- Raymond J, Roy D. Safety and efficacy of endovascular treatment of acutely ruptured aneurysms. Neurosurgery 1997;41:1235-1246 - PubMed
-
- Cognard C, Weill A, Castaings L, Rey A, Moret J. Intracranial berry aneurysms: angiographic and clinical results after endovascular treatment. Radiology 1998;206:499-510 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical